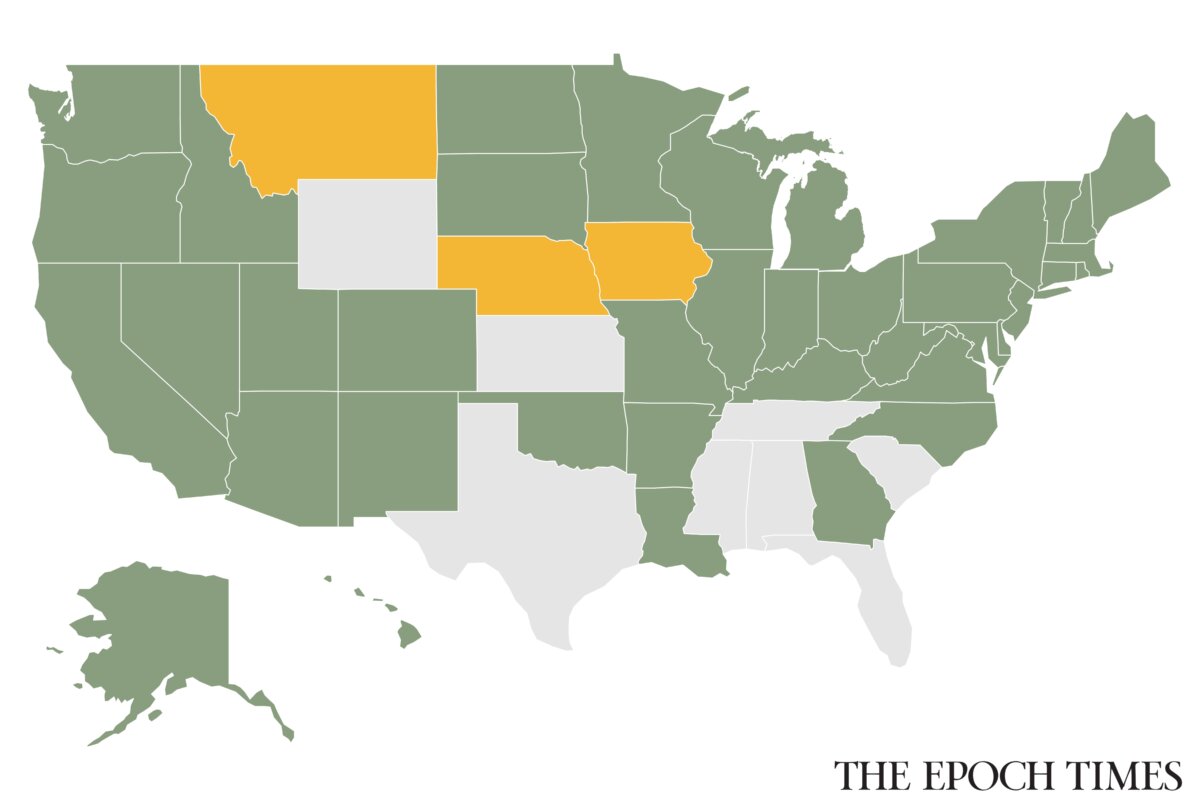

The Centers for Medicare and Medicaid Services announced new Medicaid work requirement rules for 42 states and the District of Columbia on June 1. The rules are open for comment until July 31.
The jurisdictions—which exclude Alabama, Florida, Kansas, Mississippi, South Carolina, Tennessee, Texas, and Wyoming—are those that have adopted full or partial Medicaid expansion, covering adults with incomes up to 138 percent of the federal poverty level, resulting in a coverage limit of $21,597 for an individual in 2025.
Now, those Medicaid expansion beneficiaries ages 19 to 64 must work, volunteer, or participate in job training for at least 80 hours per month, or be at least a half-time student to maintain benefits.
Individuals can also meet the requirement by earning at least 80 times the federal hourly minimum wage, which comes to $580 per month in 2026.
Once finalized, the rules will become effective on Jan. 1, 2027. However, there are exceptions.
Pregnant and postpartum women, disabled or medically frail individuals, parents and caretakers of children younger than age 14 or of people with disabilities, American Indians, and Alaska Natives are exempt from the work requirements.
States can also offer short-term hardship exceptions for people facing temporary challenges, such as receiving inpatient medical care, living in a county with unemployment at or above 8 percent, or dealing with a declared national disaster.
Some of the exemption criteria have become stricter. The age for the dependent child exclusion was 18 in the previous rule.
Also, the medically frail exclusion previously affected an individual’s Medicaid benefit package selection. Now it is used to determine whether an individual may be exempt from the work requirements.
Here are five takeaways.
Medical Frailty Defined
“The more restrictive definition of medical frailty adopted by the Trump administration will be challenging for states to implement and could lead to more people falling through the cracks and losing coverage,” said Jennifer Tolbert, deputy director at KFF, a U.S. health policy research organization.
To qualify for this exclusion, an individual must have a physical, mental, or behavioral health condition that “significantly impairs” their ability to comply with the work requirement, according to a detailed rule published on June 3.
The rule lists conditions that qualify as medical frailty: being blind or disabled; having a substance use disorder or disabling mental disorder; having a physical, intellectual, or developmental disability; or having a serious or complex medical condition—such as cancer, heart disease, or end-stage renal disease.
For those with substance use disorders, while individuals in recovery for fewer than five years can qualify as medically frail, those in “stable recovery” cannot.
The rule defines stable recovery as being in recovery for five years or longer.
“Their [conditions] are unlikely to significantly impair their ability to comply with the community engagement requirement,” the rule reads.
“We do not believe it is reasonable to categorically consider conditions as serious or complex without factoring in criteria such as the severity of the condition,” the Centers for Medicare and Medicaid Services wrote in the rule.
Stricter Limits on Self-Declaration
For now, Americans can still self-attest to an exemption on work requirements to renew their Medicaid through Dec. 31, 2027.
But beginning on Jan. 1, 2028, an individual can use a written statement, signed under penalty of perjury, to prove they are medically frail only once during their enrollment. After that, states must verify the exemption using medical claims or encounter data from the previous 12 months to renew the exemption.
If a state cannot verify the self-declared condition through its own records, the individual must provide medical documentation or a doctor’s note.
Enrollment, Spending to Decrease
The new rule will affect enrollment and spending, according to federal projections.
About 82.4 million people were enrolled in Medicaid in fiscal year 2025, including roughly 20 million adults. Total state and federal spending reached nearly $1 trillion, with about $200 billion going to the adult group.
The federal government estimated that 15 percent of adults will lose coverage because they do not meet work requirements and may not qualify for an exemption or may not submit sufficient documentation to remain covered.
The reduction in enrollment will decrease federal spending by $350 billion over 10 years, while state spending will decrease by nearly $42 billion, according to the Centers for Medicare and Medicaid Services.
Also, moving more people into the workforce will increase tax revenue, reducing annual government deficits by approximately $35 billion, the federal government stated in the rule.
Additionally, the new requirements could reduce poverty by 2.9 million people, depending on a variety of factors such as employment availability, a study from the Department of Health and Human Services suggested.
Dr. Mehmet Oz, administrator of the Centers for Medicare and Medicaid Services, said the work requirements were “historic changes” to the Medicaid program.
“This rule helps Americans build skills and independence through work, education, job training, or community service, creating new opportunities for themselves and their families,” Oz said in a statement.
While states will face some costs to build new computer systems and citizens will face a paperwork burden, these costs are very small compared with the billions saved and the economic value created, according to federal estimates.
After subtracting the costs of people’s time and the government’s administrative expenses, the country still comes out ahead by $52 billion every year, the Centers for Medicare and Medicaid Services projected.
Challenges for Medicaid Beneficiaries
Maggie Sanchez, a Medicaid beneficiary in New York City and member of the Medicaid Matters New York Steering Committee, said, “For us, Medicaid is a lifeline.”
“Many in my family have serious health concerns. What are my loved ones supposed to do if, because of these requirements, they end up with a gap in service?” Sanchez said in a statement.
“They will end up in the hospital emergency room with enormous amounts of debt. That will only lead to their mental and physical health declining even more.”
Documenting severe illnesses can be hard for some enrollees.
“We are incredibly concerned by the impact this rule could have on those struggling with cancer,” Lisa Lacasse, president of the American Cancer Society Cancer Action Network, said in a statement.
“Knowing 1 in 3 children diagnosed with the disease and 1 in 10 people with a history of cancer currently count on Medicaid for their health insurance, this coverage is a matter of life or death for millions of people nationwide.”
Lacasse said the new restrictions linking medical frailty to a person’s ability to work would mean that cancer patients and survivors would have to officially prove that they can’t work, in a process that is likely to be difficult.
Moreover, the limitation on self-reporting starting in 2028 could lead to “additional documentation and logistical challenges” for enrollees and clinicians, she said.
“Cancer will not wait while Medicaid offices sift through paperwork,” Lacasse said.
Diverse Views from Health Institutes
Since the passage of the Affordable Care Act, Medicaid has expanded dramatically among non-disabled, working-age adults, with federal matching rates seven times greater for this group than for traditional enrollees such as children, pregnant women, seniors, and people with disabilities, according to Paragon Health Institute.
“Without reforms, this distortion of state incentives crowds out care for the truly needy,” the health organization said in a statement.
Tolbert, of KFF, said the rule is “quite long and complex,” yet the implementation timeline is short.
“These challenges present risks for states given the potential for audits and financial penalties, but also for individuals who now face greater barriers to obtaining and maintaining coverage,” she said.
Ceci Connolly, president and CEO of Alliance of Community Health Plans, said: “Work and community engagement are important goals, but success of any Medicaid program should be measured by health outcomes. It would be a mistake to claim victory purely based on the number of Americans who lose coverage.”
 Friends Read Free
Copy
Facebook
Tweet
Friends Read Free
Copy
Facebook
Tweet