

Commentary
For decades, parents and doctors have sounded the alarm about the proliferation of vaccines that have been permitted on the childhood schedule. The industry that makes them has profited, but have the children become healthier? That is clearly not the case.
For perspective, and for those born after 1986, we need clarity about precisely what happened.
In 1980, American children following the Centers for Disease Control and Prevention immunization schedule received 23 vaccine doses in seven shots against seven different diseases, plus four polio vaccine drops.
In 2024, the recommended number of routine vaccines had risen to at least 84 vaccine doses in at least 57 shots for 17 diseases, plus the RSV monoclonal antibody immunization for a total of 18 diseases.
Read that again: from 23 doses to 84 doses. No other country has a schedule this outlandish.
President Donald Trump posted a provocative image that compares the number of shots in the United States with the typical number in Europe.
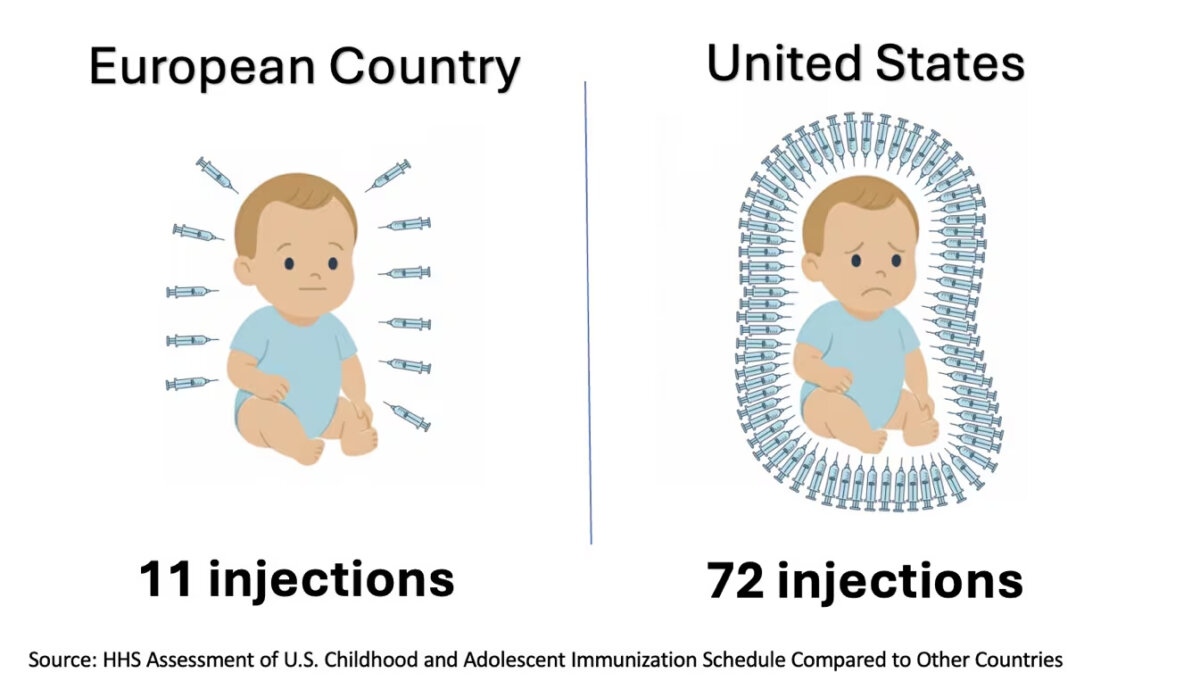
The United States injects children more than other developed nations.
Not only that, but the United States uses more coercion in injection mandates than any other nation. Most have none. In the United States, there are four states where a child is not permitted to attend school without adhering to the mandates. This is contrary to medical ethics.
The Department of Health and Human Services (HHS) has released an eye-popping report on the childhood schedule. It is signed not by some anonymous committee but by two top experts in the field.
They are Dr. Tracy Beth Hoeg, acting director of the Center for Drug Evaluation and Research, and Martin Kulldorff, chief science and data officer for the assistant secretary for planning and evaluation, who is also among the most published and cited authors on vaccines in the world.
Signing off on this document is a bold move. It reveals honesty, transparency, and tremendous confidence in the conclusions of their work. The usual academic strategy is to sign a study with as many names as possible so that no one is responsible. When trouble comes, they throw each other under the bus. That’s how it has long worked.
The usual bureaucratic strategy on documents such as this is to have only the whole committee sign, but not with names. When the trouble begins, and committee members are called, they invariably claim to have been the outlier on the committee and otherwise pressured. This happens time and again.
The authors of this study boldly stood up and said: These are our findings. If you disagree, fine, but at least you know who is to blame.
This kind of academic courage is too rare these days, especially when dealing with such a dicey topic as this.
The report pushes four core principles of a successful childhood vaccination program:
1. Scientific honesty about vaccines, including what is known and not known.
2. Informed consent; not coercion.
3. A vaccine approval process using evidence-based science and thorough post-licensure evaluation of vaccine safety and risks.
4. Recommendations that take account of the experience of peer nations.
Regarding the fourth point, the report explains:
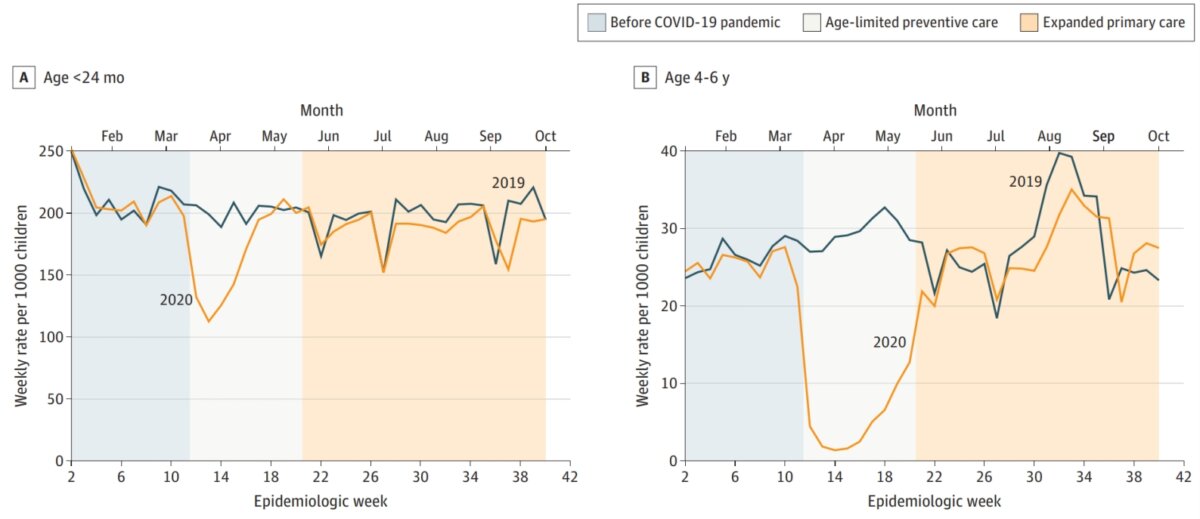
“In the decade before the COVID-19 pandemic, the U.S. had high and stable childhood vaccination rates. This changed with the pandemic lockdowns, which generated a drop in childhood vaccine uptake across all age groups (Figure 2). While the vaccination rates have rebounded, the created gaps have never been compensated for through catch-up vaccinations.”
This alone is an incredible fact. The pandemic response was driving toward inoculation of the whole population. And yet the actual reality on the ground was a dramatic decrease in routine vaccinations. Think of the irony: History’s biggest-ever push to vaccinate the population actually resulted in the opposite.
HHS has usually waited for its advisory committee on immunization practices to weigh in. This committee was deployed in the past to give some academic credibility to the Centers for Disease Control and Prevention’s recommendations. It never had power otherwise. It still remained (and remains) influential.
The committee has now met three times, and each time ended with the recommendation that the schedule be trimmed just a bit. That process has been slow, even if effective.
The new approach being pushed by HHS bypasses the committee entirely. Instead, we have two top experts weighing in with a highly competent evaluation in accordance with Trump’s wishes. Trump had said he wanted the U.S. schedule to fit with other nations. That is precisely what they have now.
The new schedule continues to recommend vaccines against some diseases, including measles, polio, and whooping cough, for all children. Immunization against six other illnesses—hepatitis A, hepatitis B, meningococcal disease, rotavirus, influenza, and respiratory syncytial virus, the leading cause of hospitalization in American infants—will be recommended for only some high-risk groups or after consultation with a health care provider.
The new schedule, in practice, will lead to a radically reduced risk for the children of adverse events related to the wild and unstudied cocktail of shots they have long been given. The remaining schedule is more in line with the evidence of safety that we have. It might still be too large a risk to take for many families.
This is why the authors of the above report are emphasizing choice as a first principle.
“While vaccine mandates may increase short-term vaccination rates, coercive measures can also have negative consequences on trust that may decrease long-term vaccination rates for consensus vaccines,” they wrote.
“It is generally considered contrary to basic medical ethics to coerce or require a medical intervention, and informed consent is a cornerstone of medical care in the U.S. and abroad.”
The report cites the Code of Medical Ethics of the American Medical Association: “Informed consent in medical treatment is fundamental in both ethics and law. Patients have the right to receive information and ask questions about recommended treatments so that they can make well-considered decisions about care. Successful communication in the patient-physician relationship fosters trust and supports shared decision making.”
It also cites the Public Health Code of Ethics of the American Public Health Association: “The effective and ethical practice of public health depends upon social and cultural conditions of respect for personal autonomy, self-determination, privacy, and the absence of domination in its many interpersonal and institutional forms.”
The coverage of the changes to the childhood schedule has been alarmist beyond all plausibility, given that the change merely aligns the U.S. schedule with international norms. The U.S. schedule blew up with proliferating shots because of the 1986 liability shield given to pharmaceutical companies. If a shot landed on the childhood schedule, the company could rest easy in complete indemnification regarding any harms.
It is highly likely that this shield will be affected profoundly by the new exclusions from the schedule. The shotmakers might be facing some seriously profound litigation in the future.
We can look forward to other changes coming in the next year.
1. Composite shots will have to be divided into single-disease inoculations, so measles, mumps, and rubella will be given separately.
2. The cocktail mix of shots has never been studied in randomized controlled trials, so such trials will be made essential.
3. The liability shield will be revisited.
4. The Supreme Court is likely to rule against shot mandates that violate ethical codes.
5. Pharmaceutical companies will have to produce evidence of safety in post-marketing trials, else see their products taken off the market.
This is just the beginning of the changes that are coming. In the backdrop of all this new focus is, of course, the experience of the 2020 pandemic response, which was all about getting shots in arms. Government officials even removed proven therapeutics from shelves to prepare the way.
That experience was a trauma for everyone. There has never been a commission to revisit this period and likely will never be. But in the reforms unfolding now, we are seeing a response of sorts. The power of the pharmaceutical companies and their largely unquestioned hold over public health is finally facing a serious reckoning.
Views expressed in this article are the opinions of the author and do not necessarily reflect the views of The Epoch Times.
 Friends Read Free
Copy
Facebook
Tweet
Friends Read Free
Copy
Facebook
Tweet




























