Prescription drug prices charged by hospitals vary by thousands of dollars for the same medication, depending on where the hospital is located and who’s paying, according to a study published by Patients Rights Advocacy.
The confusing price structures are often available only in computer files that are unusable by average consumers, despite federal transparency rules.
That makes it virtually impossible for patients to make informed decisions on where to go for health care, according to the report’s producer, 3 Axis Advisors.
“The U.S. prescription drug supply chain suffers from a pricing problem,” Antonio Ciaccia, President of 3 Axis Advisors, told The Epoch Times. “The hospitals and the pharmacies and the manufacturers set prices that are aspirational.”
The actual prices are negotiated through discounts and rebates that may be dramatically lower than the sticker price, or, in some cases, higher.
Here’s what analysts discovered about hospital pricing patterns for prescription drugs after analyzing 1,300 publicly available master price files.
Prices Vary Widely
Hospitals normally list three prices for a drug: the list price, the cash price paid by people without insurance, and the negotiated prices paid by various insurance companies.
That means there are multiple prices for every drug, depending on whether the patient pays cash or is covered by insurance. Even insured patients may pay widely different prices, depending on the discount negotiated by their insurance company.
For a given drug, there may be as many as a dozen different prices charged at the same facility, depending on who’s paying.
The difference can be significant. The greatest price difference analysts observed for a single drug within one hospital was 1-to-2,347. That means a product for which one patient may be charged $1 could cost another patient $2,347.
“Whatever is happening right now isn’t working, and it certainly wouldn’t be constituted as fair, and it certainly wouldn’t be necessarily traditional laws of supply and demand,” Ciaccia said.
Data Little Help to Consumers
President Donald Trump instituted federal rules mandating price transparency for hospitals in 2019. Hospitals must make their standard charges for all items and services available to the public in machine-readable files.
Most consumers don’t have access to usable price information. That’s partly because the regulation is not always followed. Analysts found that 7 percent of the files analyzed did not contain properly formatted information. And only 63 percent contained usable price information.
Some hospitals present their information in a format that is not easily understood by laypeople. Others present the information in spreadsheet form, but the files are very large and not easily handled.
The Epoch Times downloaded several hospital price files.
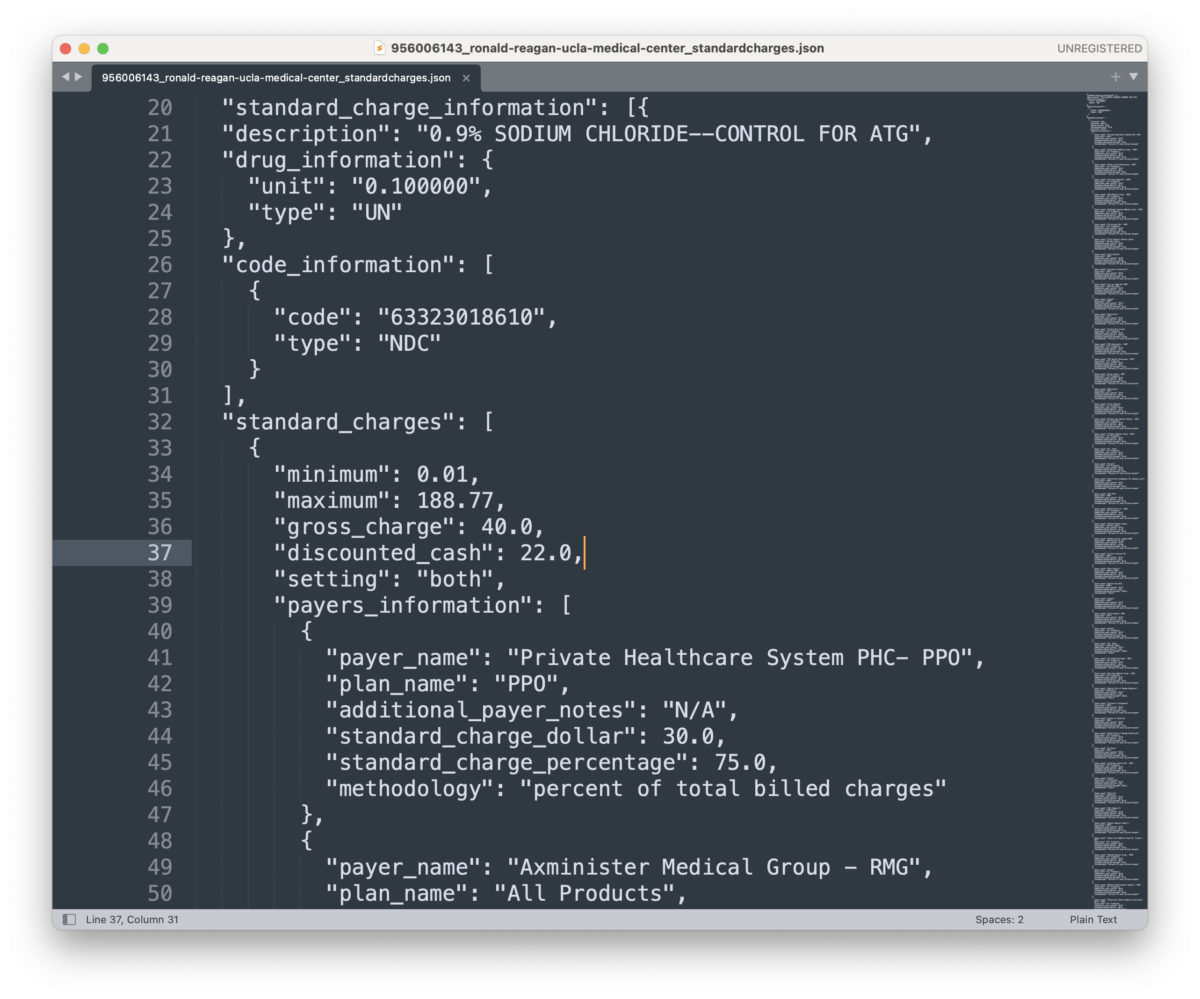
A file from UCLA Health was presented in JSON format, which can be read with a text editing application. However, the format may be confusing to many consumers.
A file from Trinity Health Ann Arbor Hospital was available in a spreadsheet-compatible format. However, the 5-gigabyte file contained more than 15 million rows and could not be accessed using Microsoft Excel or Google Sheets on a standard laptop computer.
“When the same drug or healthcare service can have a dozen different prices from the same provider on the same day, it becomes difficult to argue that there is a defined price for that product or service at that location,” the report authors concluded.
Flying Cross Country Offers Savings
List prices for pharmaceutical products are highly inflated, according to Ciaccia. Consumers have little leverage in negotiating a better deal, while insurance companies have significantly more.
The average insurance company discount is about 40 percent off the list price, but there are wide variations.
The report cited data showing that hospital systems that have a monopoly in the marketplace charge an average of 12 percent more than those in markets with four or more providers.
For example, patients purchasing cancer drug Opdivo with the insurance company Medica are charged $17,217, on average, at hospitals in Massachusetts and $66,855 in Colorado.
Patients covered by UnitedHealthCare are charged an average of $12,059 for immunotherapy medication Keytruda in Colorado, but $43,099 in Massachusetts.
“On average, there is over a $35,000 difference in therapy cost depending upon which hospital one of these medications is received at, even if the insurance carrier managing the payment rate of the drug is fixed,” the report stated, referring to five medications selected for particular analysis.
In some cases, a patient might be able to travel cross-country to receive treatment and still save money, the authors concluded.
Transparency as a Starting Point
Price transparency is the starting point for creating solutions, Ciaccia said. “Diagnose and then treat. Now we know the prices. The question is, ‘how do we weaponize that information to create a more efficient marketplace?”
Ciaccia noted that Mark Cuban’s Cost Plus Drug Company publishes each drug’s cost and a 15 percent markup. “The prices are the same for everybody,” Ciaccia said.
“The beauty of price transparency is that now we have an understanding of what the same drugs are being sold for in other areas. The question then becomes, why is it so disparate? And are there policy mechanisms that can better help create efficiencies in that marketplace?”
Ciaccia said he doesn’t know, but thinks getting clear, usable price information is the place to start.
The Epoch Times requested comments from the American Hospital Association, United Healthcare, and Pharmaceutical Research and Manufacturers of America, but no responses were received by the time of publication.
 Friends Read Free
Copy
Facebook
Tweet
Friends Read Free
Copy
Facebook
Tweet