

Trampus Braaten, 45, kept showing up with the same questions. Why did he have dizziness, then headaches, then vertigo so severe that he couldn’t drive?
The emergency room ruled out immediate threats. Visits with his primary care doctor were brief, followed by referrals to specialists that pushed appointments weeks into the future. Each one required him to begin again, retelling the story to someone new. Nearly three months passed like this. The symptoms didn’t change.
Braaten kept returning, carrying the details with him as uncertainty gave way to anxiety. Eventually, one doctor paused long enough to hear the pattern. The diagnosis—vestibular neuritis, inflammation of the balance nerve in the inner ear—came late, but it brought relief.
By then, he had already learned how much effort it took to stay visible.
The 15-Minute Reality
In U.S. health care today, a single doctor rarely follows a patient’s story from start to finish.
Primary care visits are scheduled for 15 to 30 minutes, most offering a little more than 15 minutes of face time. In that sliver, doctors must listen to symptoms, perform an exam, review records, diagnose, order tests, adjust medications, explain everything, and document it all.
Care has also grown more diffuse. Specialization has expanded, sending patients from one doctor to the next, while their records scatter across systems that don’t reliably communicate.
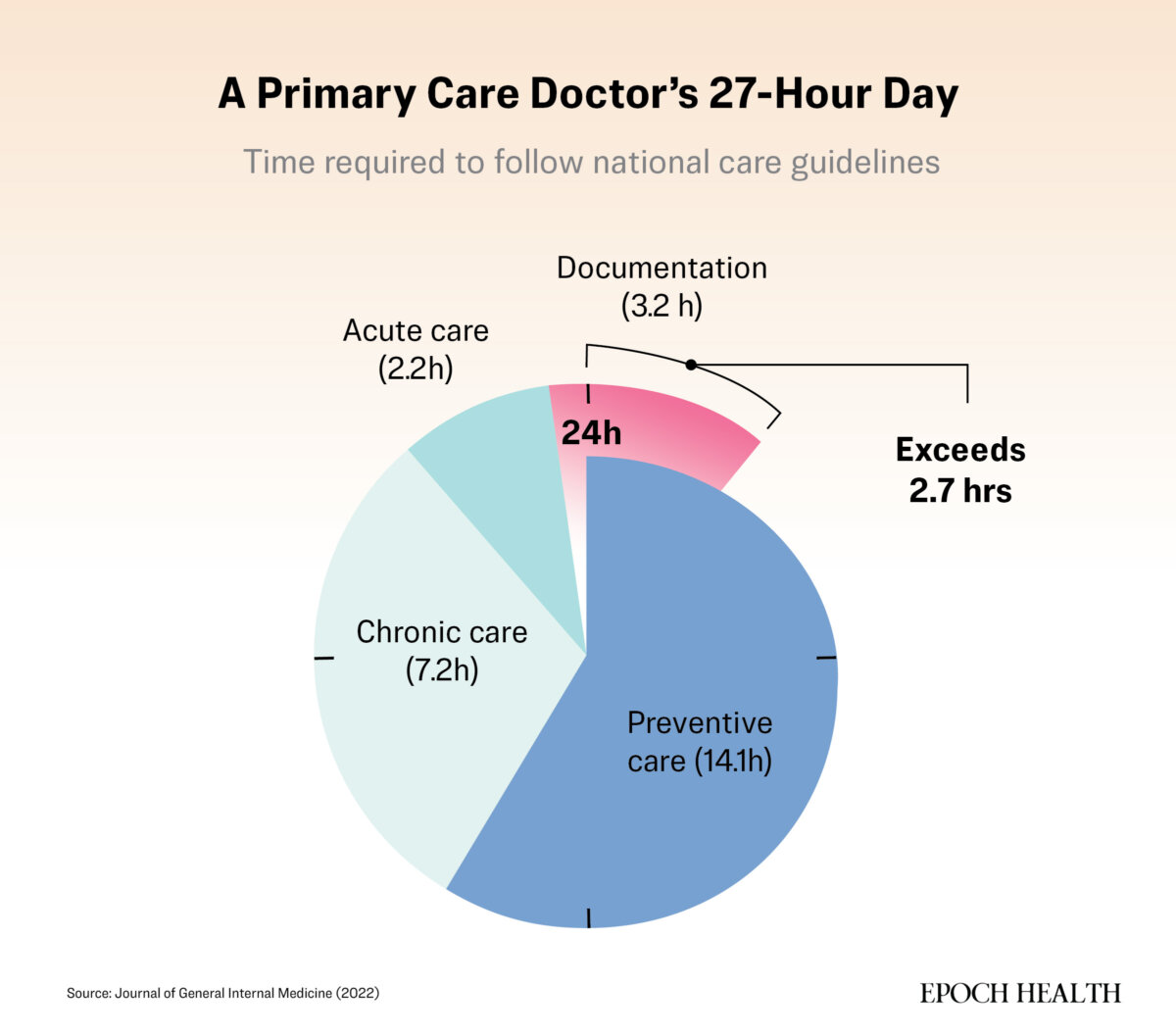
Patients feel the squeeze. Millions of people leave visits unsure of what they were told or what comes next. A 2022 simulation study published in the Journal of General Internal Medicine estimated that to deliver all guideline-recommended preventive, chronic, and acute care to all their patients, a primary care doctor would need 27 hours per day.
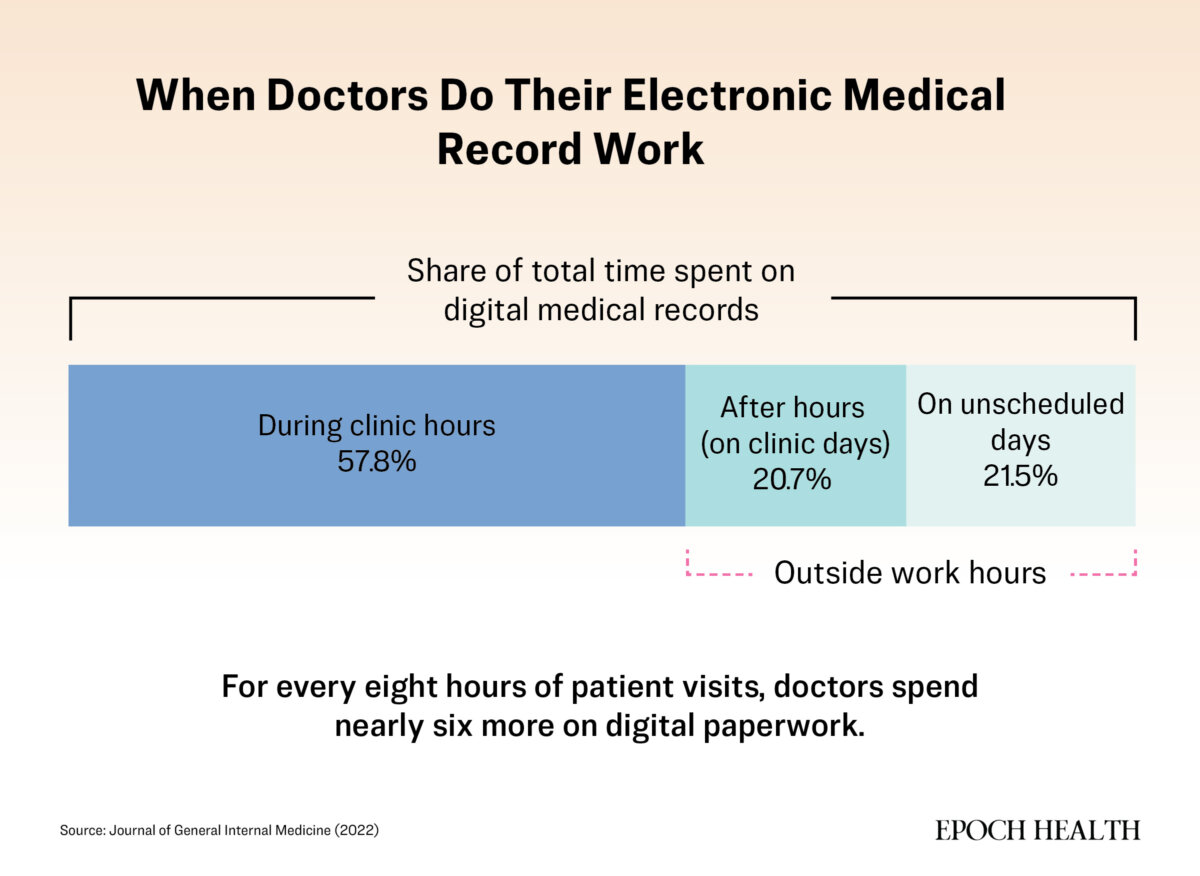
Time doesn’t just fall short in the exam room. For every hour with patients, doctors spend nearly another hour on paperwork—much of it uncompensated.
“Good care takes time,” Dr. Victoria Sweet, author of “Slow Medicine,” told The Epoch Times.
Instead, she said, doctors are expected to do too much, too fast, with too little support.
What is often lost is context: how a patient lives, what they can manage, and what worries them most. Diagnoses are made and orders placed, but the broader story remains incomplete.
Across millions of visits, the effects add up. In 2024, a major international analysis ranked the United States last among 10 high-income nations in overall health system performance, despite spending more per person than any peer.
When the Dots Don’t Connect
Today, about one in three Medicare patients sees five or more doctors per year—up sharply since 2000. On average, a family doctor’s Medicare patients collectively received care from roughly 50 other doctors (mostly specialists) in 2000. By 2019, that number had nearly doubled to about 95. That means family doctors must now track nearly twice as many specialists to keep care from falling apart.
As patients move between clinicians and care settings, responsibility thins. The Joint Commission, which accredits U.S. hospitals and health systems, states that nearly two-thirds of serious adverse medical events stem from communication failures during care transitions.
“We’ve replaced people with processes,” Dr. Marc Lato, a family physician and former medical director, told The Epoch Times. “There’s a process for everything, but not one person who really knows you.”
Electronic records were supposed to bridge the gap. Instead, notes go unread, results get buried, and systems still don’t speak to one another. Your story ends up scattered across half a dozen portals.
The fallout is concrete. Studies show abnormal test results routinely go uncommunicated—especially after emergency department visits or specialist consultations. Follow-up on imaging or laboratory results now frequently requires the patient to notice and chase.
It happens every day: Blood work ordered in the ER posts days later to a portal—flagged abnormal, not urgent. No one calls. The ER doctor has rotated off. The primary-care doctor never sees it because it lives in a different system. Weeks pass. The patient assumes no news is good news.
When symptoms finally force a return visit, the abnormality has progressed—not because anyone was negligent, but because no one assumed responsibility for the follow-up.
That responsibility now defaults to you.
What Patients Don’t See
Most patients assume decisions stem solely from medical judgment. In reality, they are shaped by forces rarely visible in the exam room.
Care is increasingly influenced by ownership and finance—private equity firms and corporations buy clinics, staffing models, even diagnostic tools, according to Sweet. Patients see a physician in the room, she said, but the incentives shaping that visit often originate elsewhere.
Payment structures reveal this most clearly. Most U.S. physicians are reimbursed by task, not outcome. Visits, tests, and procedures generate revenue; thinking, coordinating, or following up often does not. A deep diagnostic conversation may pay less than a battery of tests.
When a chart opens, billing prompts and documentation demands appear. The visit becomes a negotiation between patient needs and system requirements.
“In 15 minutes, you’re not treating a person. You’re checking boxes,” Dr. Andy Lazris, a geriatrician and author, told The Epoch Times. “We get paid when we do the checklist.”
Incentives can affect which drug is prescribed, how aggressively a test is pursued, or how long a visit lasts, often without being explicitly acknowledged. Under Medicare, procedures are reimbursed at five or 10 times the rate of a consultation, regardless of whether it improves a patient’s life. Whether a patient actually gets better is rarely tracked or rewarded.
Fear amplifies “just in case” testing. Nearly one in three U.S. physicians has been sued, although most claims fail. Defensive medicine fills spaces where trust and continuity once stood.
Why the Failures Are Not About Blame
“It’s not that your doctor doesn’t care,” Lazris said.
The problem is misalignment. The system rewards documentation and volume, not listening or thinking.
Physicians feel the same pull their patients do—the constant tug away from the work that drew them to medicine in the first place.
“There’s a sense of physicians feeling the additional burden from what they would prefer to do,” Dr. Zeke Silva, who chairs the American Medical Association’s Relative Value Scale Update Committee, told The Epoch Times. “Which is interface with their patient, help their patient, learn from their patient.”
The American Medical Association has long advocated for better pay for care that happens outside the exam room, including follow-ups, coordination, phone calls, and chart reviews. Progress has been slow.
The result is shared frustration. Patients leave feeling unseen, and doctors leave feeling constrained. The system registers neither.
[series_posts_list][/series_posts_list]
What Patient Engagement Now Means
In theory, patients are free to stay passive. In practice, passivity has become a clinical risk.
“The best relationships are partnerships,” Dr. Dorothy Serna, an internal medicine physician, told The Epoch Times. “The people who do best are the ones who take agency.”
That may mean confirming that a referral went through, asking what happens if a test is abnormal, and circling back when no one calls about results.
“If something doesn’t happen,” Serna said, “you’re the one who lives with the consequences.”
Engagement doesn’t guarantee perfect outcomes. The system can still fail even the most vigilant patient—but evidence shows it steadily improves the odds.
The harder truth is that not everyone can self-advocate. Nearly nine in 10 U.S. adults have limited health literacy, struggling to understand instructions, read portals, or navigate referrals. Older adults, people with cognitive challenges, language barriers, multiple jobs, or serious chronic illness carry the heaviest load in a system that now relies on patient vigilance to catch gaps.
A system that requires self-advocacy rewards the resourced and penalizes the vulnerable.
Medicine Is Built for Crises, Not Lives
Modern medicine shines in emergencies. It can restart hearts, dissolve clots, and stabilize trauma. Excellence reflects its core design—treating acute, fixable problems with clear endpoints.
Chronic illness refuses that script. It unfolds slowly, shaped by sleep, stress, diet, movement, environment, and daily habits. Symptoms shift week to week, sometimes day to day. It rarely announces itself with drama and seldom fits neatly into billing codes or 15-minute slots.
Sweet said this mismatch drives much of patients’ frustration. Medicine often treats the body as a machine, in which a broken part can be fixed or replaced. Most physicians get little formal training in nutrition, behavior modification, or long-term coaching. They aren’t paid to guide habits over months or years. They rarely get the time.
“There’s this idea the doctor knows best,” Sweet said. “But patients know things too.”
What This Moment Demands
In today’s medicine, patient silence is no longer safe. It carries real clinical risk.
You do not need to become an expert. You need to remain present. Notice when something doesn’t add up, ask what happens next—and what happens if nothing happens at all.
You didn’t go to medical school, but you are the only person who has been in the room for every single moment of your care. That makes you the through-line—the one constant—in a system built entirely on handoffs.
Tools from earlier in this series—preparing sharp questions for brief visits, tracking your own lab results over time, knowing when to seek a second opinion, stepping back from cascades, questioning routine screenings—are now core defenses. Passivity, once merely inconvenient, has become a clinical hazard.
What to Carry Forward
- The System’s Failures Are Structural, Not Personal: Short visits, fragmented care, and rushed decisions flow directly from how medicine is organized and paid for.
- No Clinician Sees the Full Picture: Across handoffs and specialties, you may be the only constant.
- Engagement Is Now Protective: Not optional, not ideal—protective.
- Health Is Shaped Mostly Outside the Exam Room: What happens between visits often matters as much as what happens inside.
- Agency Isn’t Expertise: You didn’t design this system, and you don’t need to become a medical expert to navigate it. Stay present, curious, and willing to speak up when something doesn’t make sense.
None of this implies the system is unchangeable.
Some practices are already showing a different path forward. Models such as integrated health systems, concierge medicine, and direct primary care—where patients pay a membership fee for more personalized, longer visits—focus on deeper relationships and continuity of care rather than seeing as many patients as possible.
From 2018 to 2023, the number of direct primary care sites increased by 83 percent, and the number of clinicians working in them rose by 78 percent.
Integrated health systems and concierge practices follow similar models, prioritizing relationships over throughput.
These options remain exceptions, not the rule. Most patients still navigate systems that were never designed for complexity, continuity, or time.
Until that changes, engagement has become protective— not because it’s fair but because it’s necessary.
What’s Next: How to think clearly about alternative care models when standard medicine falls short, and how to decide what’s worth pursuing, and what isn’t.