

According to the recommendations from the Centers for Disease Control and Prevention (CDC) and the Food and Drug Administration (FDA), pregnant women should be vaccinated against COVID-19. However, the main research work to back up this policy was the influential CDC-sponsored article by Shimabukuro et al. (2021), published in the New England Journal of Medicine, which has been corrected after wide criticism. In the published correction, the authors stated that “No denominator was available to calculate a risk estimate for spontaneous abortions because, at the time of this report, follow-up through 20 weeks was not yet available for 905 of the 1224 participants vaccinated within 30 days before the first day of the last menstrual period or in the first trimester. Furthermore, any risk estimate would need to account for the gestational week–specific risk of spontaneous abortion.”
Therefore, there is essentially little assurance of the COVID-19 vaccine safety on women during pregnancy, particularly for those exposed in early pregnancy in their first trimester. But the article’s abstract and conclusions did not reflect the correction regarding the risks in the first trimester, and neither did CDC change its policy accordingly.
Although many doctors have called for a halt to COVID-19 vaccination for pregnant women since last year, the CDC and FDA have never responded to this officially. Recently, in an educational conference hosted by Front Line COVID-19 Critical Care Alliance (FLCCC Alliance), Dr. James Thorp, a renowned obstetrician, and gynecologist, presented additional observations regarding some vaccine-related risks for pregnant mothers, their fetuses, and even newborn babies when taking milk from vaccinated mothers. Some of his patients have also come to him for help after experiencing different side effects after their vaccination.
One important cohort study that Dr. Thorp highlighted in his speech found that among its 11 participants, who were lactating mothers, mRNA from COVID-19 vaccines was found in the breast milk of five individuals, accounting for 45 percent of the entire cohort. These participants received the vaccination within six months of their delivery.
Dr. Thorp has seen at least three newborns, who were completely healthy at the time of their birth, who passed away after being breastfed by their recently vaccinated mothers. Of course, these examples cannot prove a causal relationship between the COVID-19 vaccines and the infants’ deaths. However, the observation that the mRNA from the COVID-19 vaccine existed in the breast milk of lactating mothers suggested that mRNA vaccine components can not only accumulate in ovaries in females but also have the potential to be passed onto infants via breastfeeding. Therefore, this issue should be raised to the public to warn people about the potential risks. Further investigations need to be carried out to find the reasons behind these deaths.
Mothers’ vaccination may also negatively affect their unborn fetuses. Judicial Watch, a foundation focusing on accountability and integrity in law, politics, and the government, has obtained the trial data from Moderna’s COVID-19 vaccine animal experiments, thanks to the Freedom of Information Act. Moderna conducted these experiments to meet the FDA’s reproductive toxicology requirement. According to these Moderna documents, some lab rat fetuses ended up with malformed wavy ribs, after their mothers’ vaccination, with a fetal prevalence of 4.03 percent.
These experiments have also shown that the COVID-19 vaccines’ mRNA and spike protein can travel through all barriers in a mother rat to enter its fetus. Furthermore, mother rats experienced toxicity during gestation, and a high level of antigens was found in their bodies. This implies that their bodies had become toxic. In addition, the vaccines could cause the rats to lose their fertility and their ability to use their hind legs.
Some bone malformations can even be lethal. Again, although clinically speaking, it cannot be proven that the COVID-19 vaccines have caused deadly fetal malformation, however, the mothers of such deformed and deceased infants did receive COVID-19 vaccines before such conditions developed.
COVID-19 Vaccines Might be Related to Altered Menstrual Patterns and Other Adverse Events
A paper authored by Dr. Thorp and his colleagues and posted on Preprints.org, a preprint server, compared the relative rates of adverse event reports between COVID-19 and seasonal influenza vaccines. These adverse events occurred after vaccination, although causational relationships have not been verified.
In this paper, a relative rate (RR value) greater than 1 means that more adverse events are reported after COVID-19 vaccinations than flu vaccinations. Among all the listed adverse events, menstrual abnormality has a RR value of 1192, ranking at the top. The other listed adverse events, including miscarriage, fetal malformation, and fetal cardiac disease, all have a RR value greater than 1.
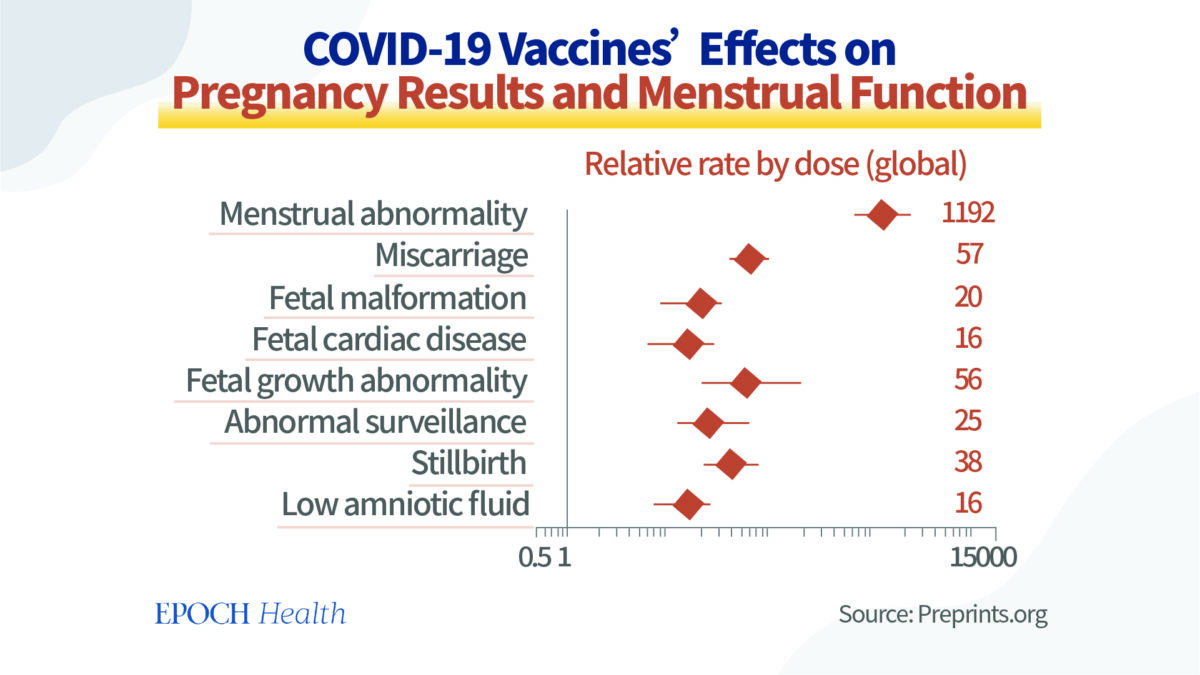
Therefore, in comparison with the influenza vaccines, COVID-19 vaccines are associated with a significant increase in adverse events, including menstrual abnormality, miscarriage, fetal chromosomal abnormalities, fetal malformation, fetal cardiac disorders, fetal growth abnormalities, fetal placental thrombosis, and fetal death and stillbirth.
Given such a long list of serious adverse events, Dr. Thorp once again called for a halt to the recommendation of COVID-19 vaccines for pregnant women, until long-term data becomes available.
Since 2021, many people have been reporting that unexpected menstrual patterns started taking place after their COVID-19 vaccination, including people who had had menopause.
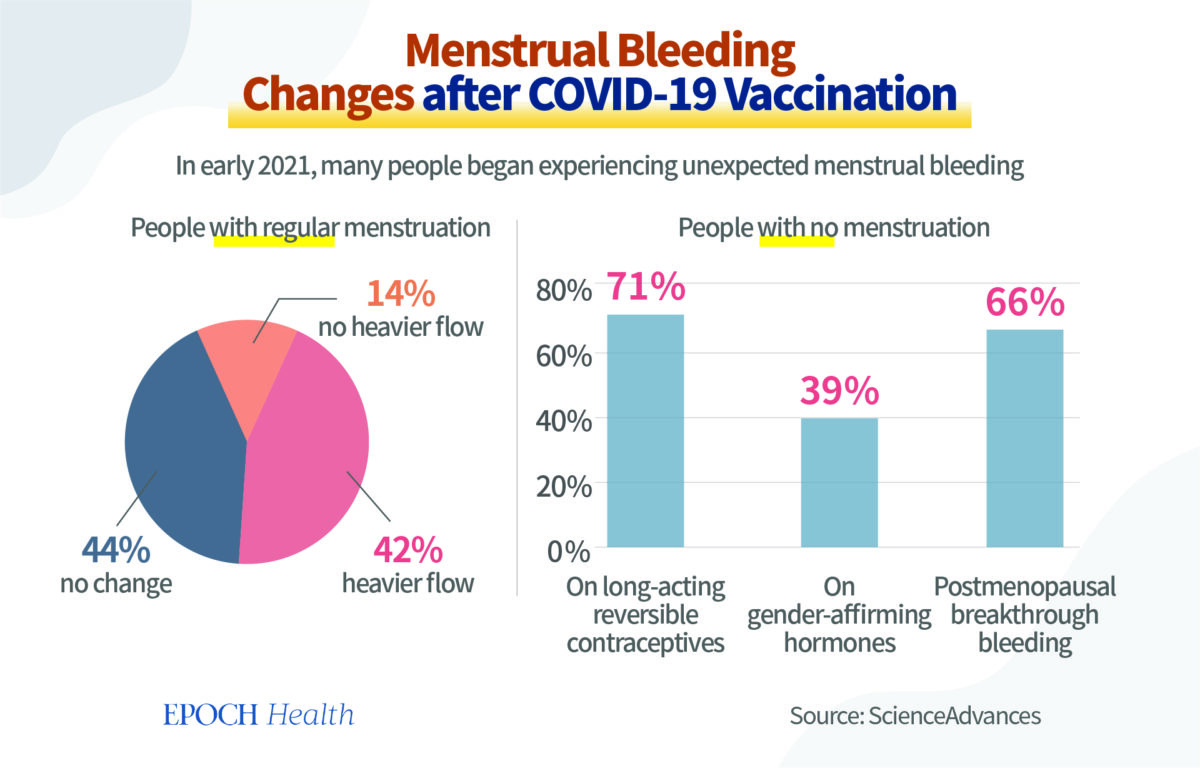
For people who had a regular menstrual cycle before their vaccination, 42 percent started to bleed more heavily than before, 44 percent had no change, and 14 percent didn’t experience an increase in menstrual flow. Of course, to females, the heavier the menstrual flow, the more damage it causes to their bodies.
For people who typically didn’t have menstrual cycles, 71 percent were using long-acting reversible contraceptives, 39 percent were undergoing gender-affirming hormone therapies, and 66 percent were postmenopausal people reporting breakthrough bleeding.
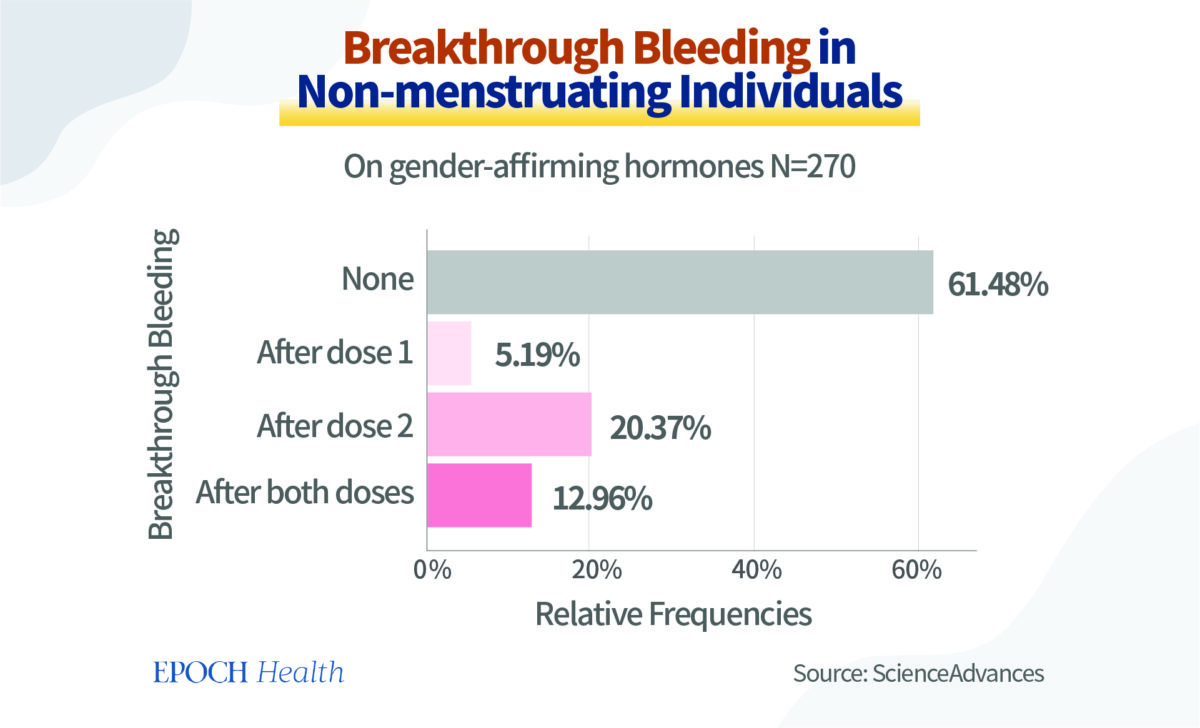
Among 270 vaccinated people who were on gender-affirming hormone therapies and had breakthrough bleeding, in 20.37 percent of the cases, their breakthrough bleeding took place after the second dose of vaccination; and in another 12.96 percent of the cases, their breakthrough bleeding occurred after both doses.
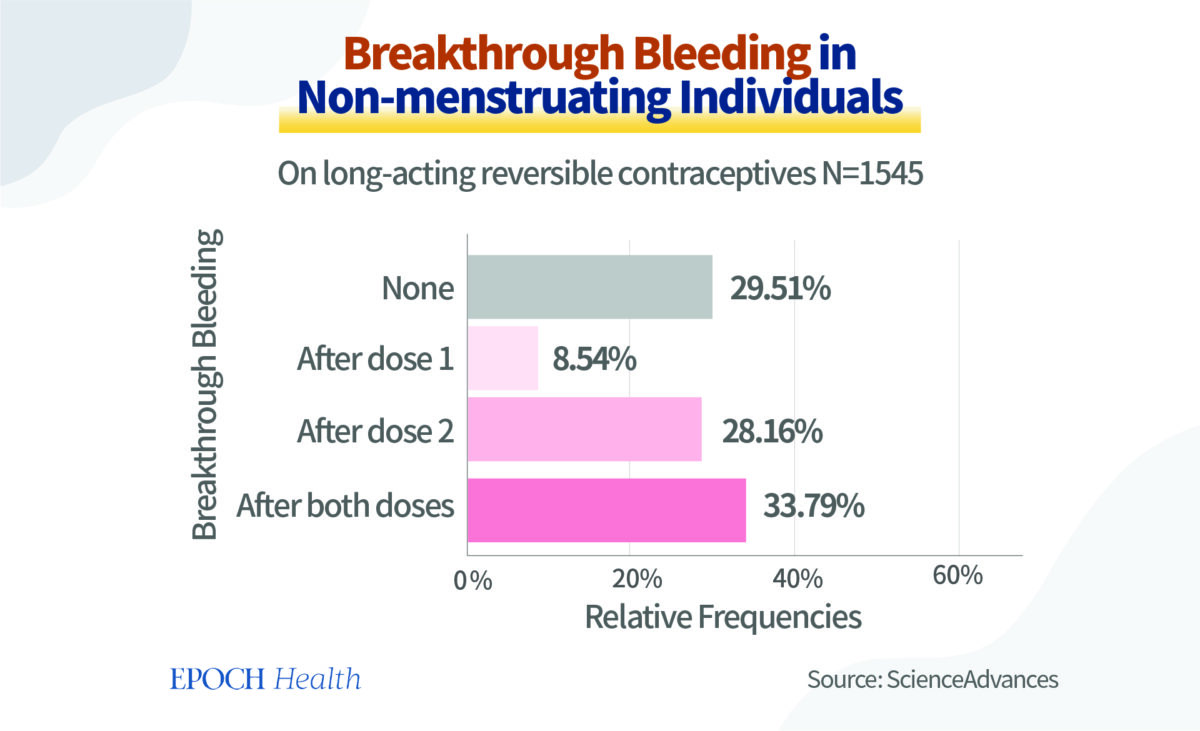
Among 1,545 vaccinated people who were on long-acting reversible contraceptives and had breakthrough bleeding, in 28.16 percent of the cases, their breakthrough bleeding took place after the second dose of vaccine; and in another 33.79 percent of the cases, their breakthrough bleeding occurred after both doses.
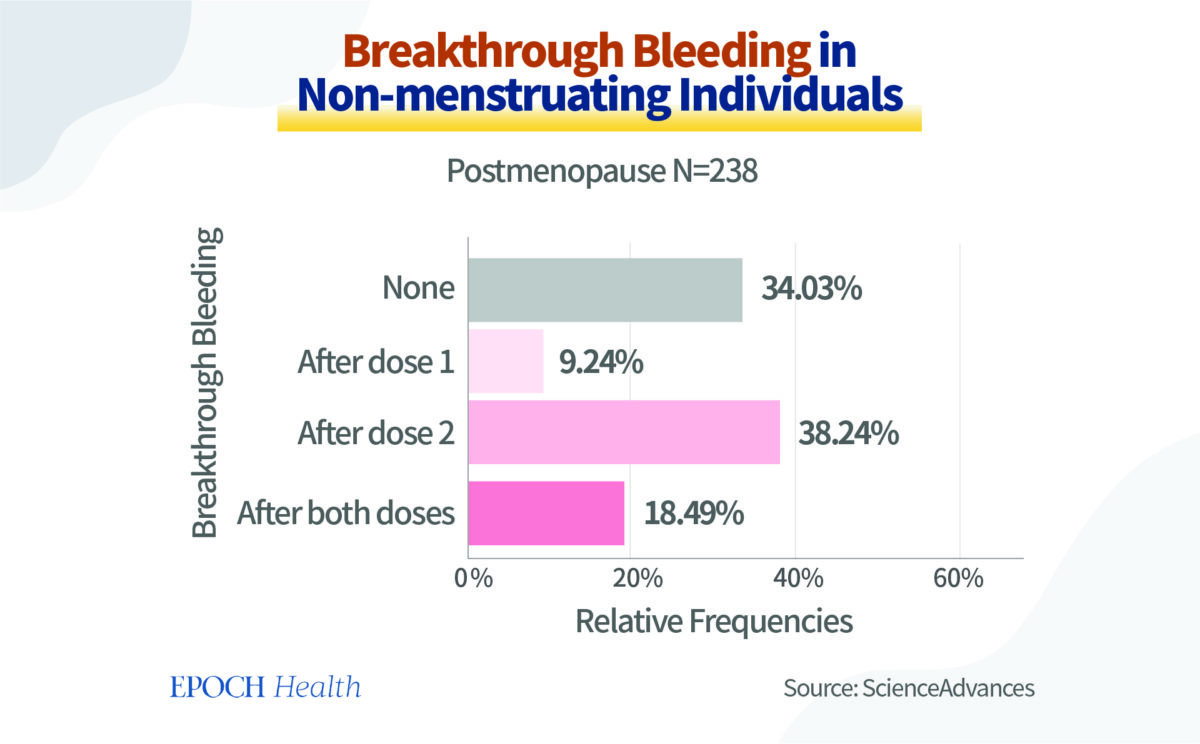
Among 238 vaccinated people who had had menopause in the past and had breakthrough bleeding, in 38.24 percent of the cases, their breakthrough bleeding took place after the second dose of vaccine; and in another 18.49 percent of the cases, their breakthrough bleeding occurred after both doses.
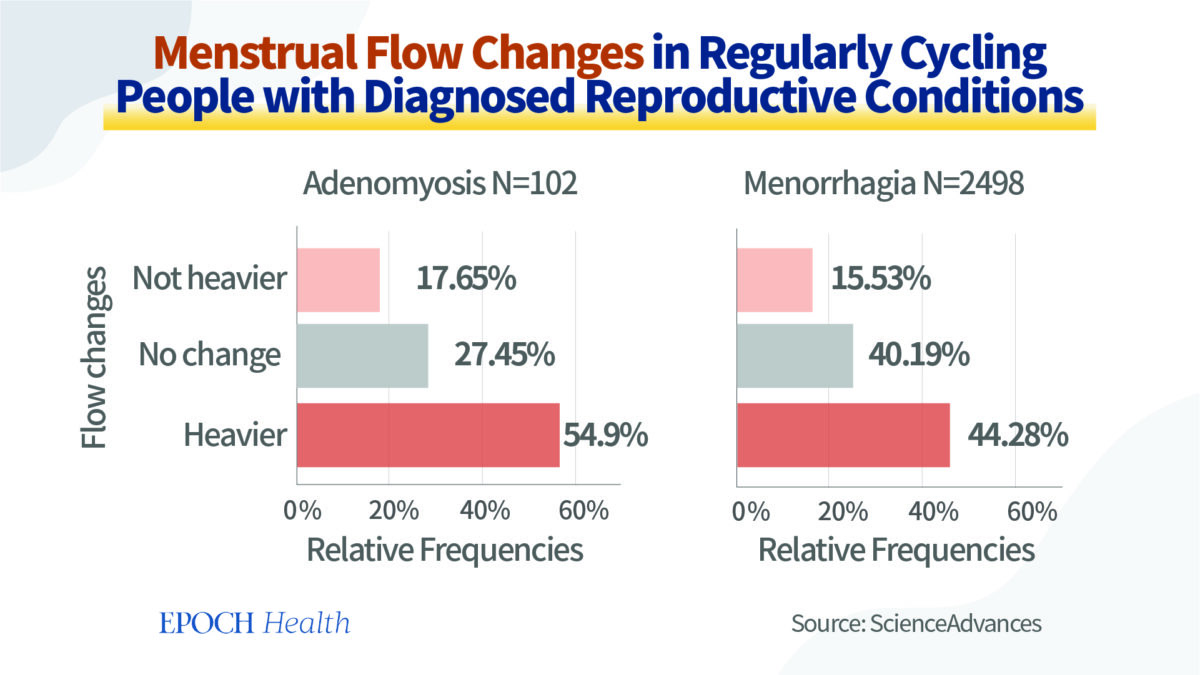
Among 102 people who had regular menstrual cycles and adenomyosis, after vaccination, 54.9 percent had a heavier flow, while another 27.45 percent reported no change in menstrual flow.
And among 2,498 people who had regular menstrual cycles and menorrhagia, after vaccination, 44.28 percent had a heavier flow, while another 40.19 percent reported no change.
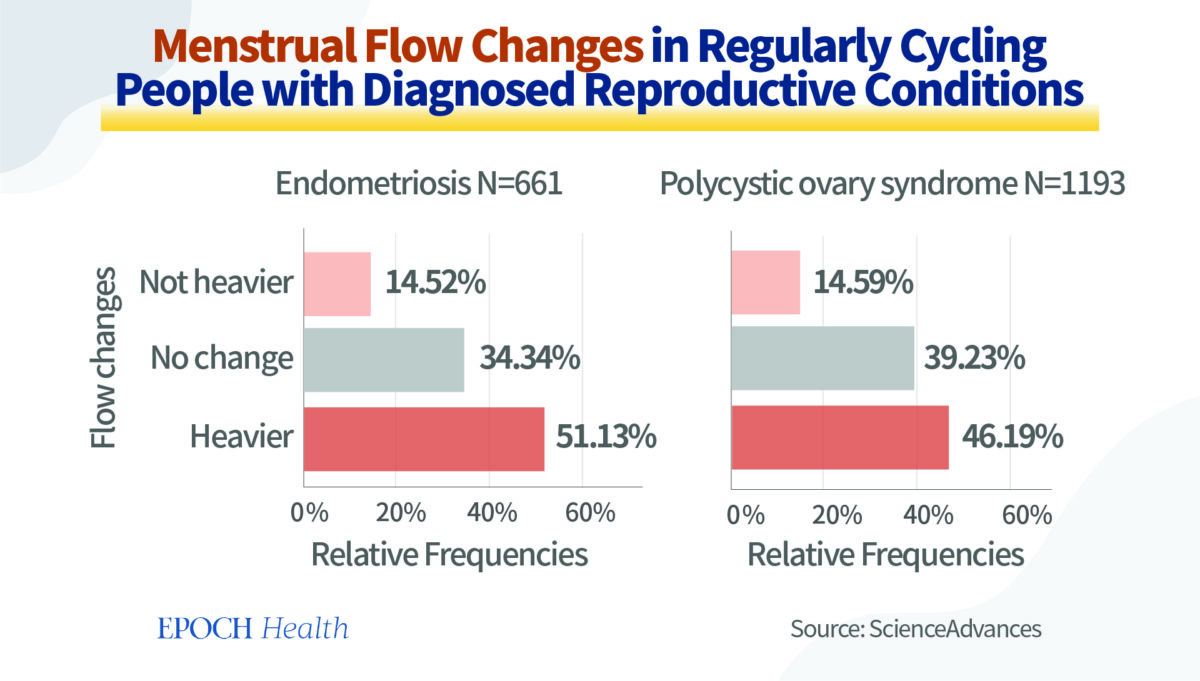
Among 661 people who had regular menstrual cycles and endometriosis, after vaccination, 51.13 percent had a heavier flow, while another 34.34 percent reported no change in menstrual flow.
Among 1,193 people who had regular menstrual cycles and polycystic ovary syndrome (PCOS), after vaccination, 46.19 percent had a heavier flow, while another 39.23 percent reported no change.
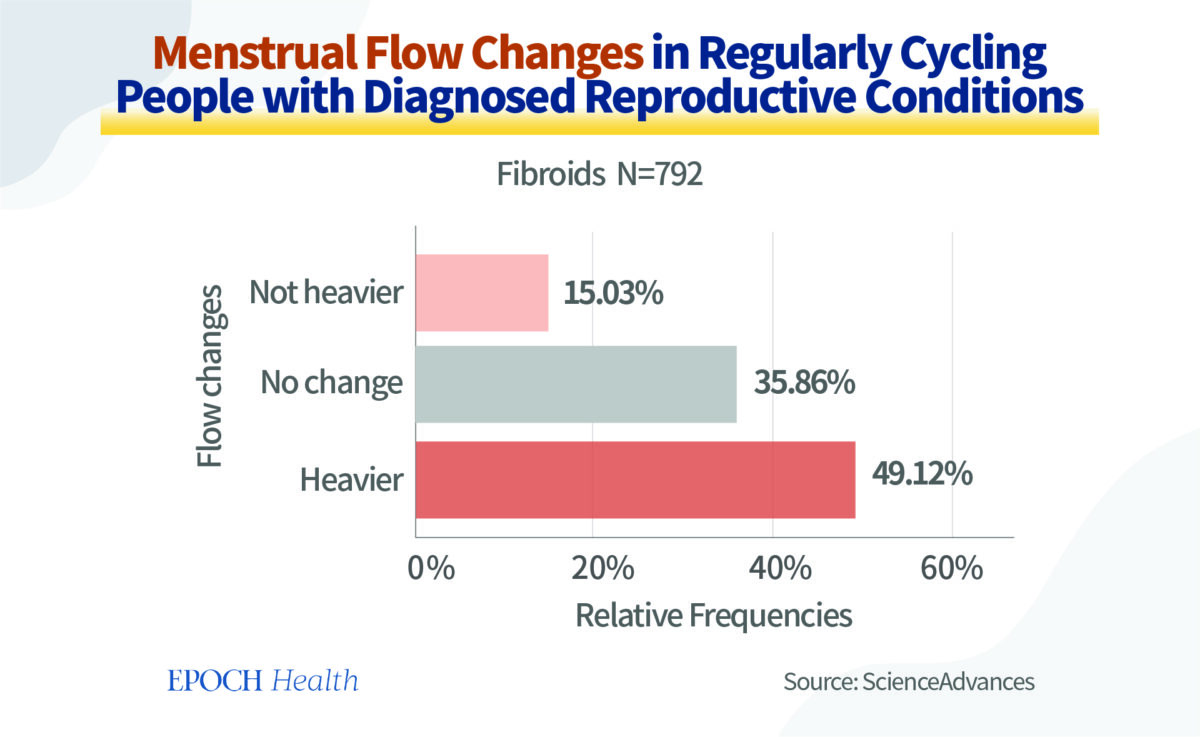
Among 792 people who had regular menstrual cycles and fibroids, after vaccination, 49.12 percent had a heavier flow, while another 35.86 percent reported no change.
Therefore, although the purpose of receiving COVID-19 vaccines is to prevent COVID-19 infection, these components of the vaccines can affect the frequency and volume of females’ menstrual flows. For people who have underlying diseases such as endometriosis and PCOS, the changes in their menstrual flows would become more obvious than for people who don’t have underlying conditions. As their reproductive systems are affected, the secretion of their hormones, in general, would also become affected.
These observations suggested that the COVID-19 vaccination is associated with significant changes in the production and secretion of hormones, and/or the regulation of menstrual cycles in women’s bodies. As there are no long-term follow-up studies for these women who suffered from these adverse events, it is not clear whether there are potential long-term injuries or permanent damages to the female reproductive system. It is possible that when the spike proteins and the related lipid nanoparticles are cleared from the ovaries, the adverse effects would stop. However, more long-term studies are needed to confirm this.
A Surge of Decidual Cast Shedding Has Been Reported Since COVID-19 Vaccination Started
According to another paper by Dr. James Thorp, Tiffany Parotto, and their colleagues, there was a sharp rise of decidual cast shedding (DCS) cases taking place in 2021, after the implementation of COVID-19 vaccines.
DCS has previously been considered a rare gynecological condition. It takes place when the uterus’s mucous lining sheds intact with a shape similar to that of the uterine cavity, and the “cast” made from this process is triangular. Less than 40 DCS cases were reported over the last 109 years. However, during the 7.5-month period from May 16 to December 31, 2021, at least 202 women experienced this condition.
Tiffany Parotto is the CEO and president of MyCycleStory.com, an independent research study collecting data about women’s irregular menstrual experiences since the use of COVID-19 vaccines in an effort to understand these vaccines’ potential effects on the female body.
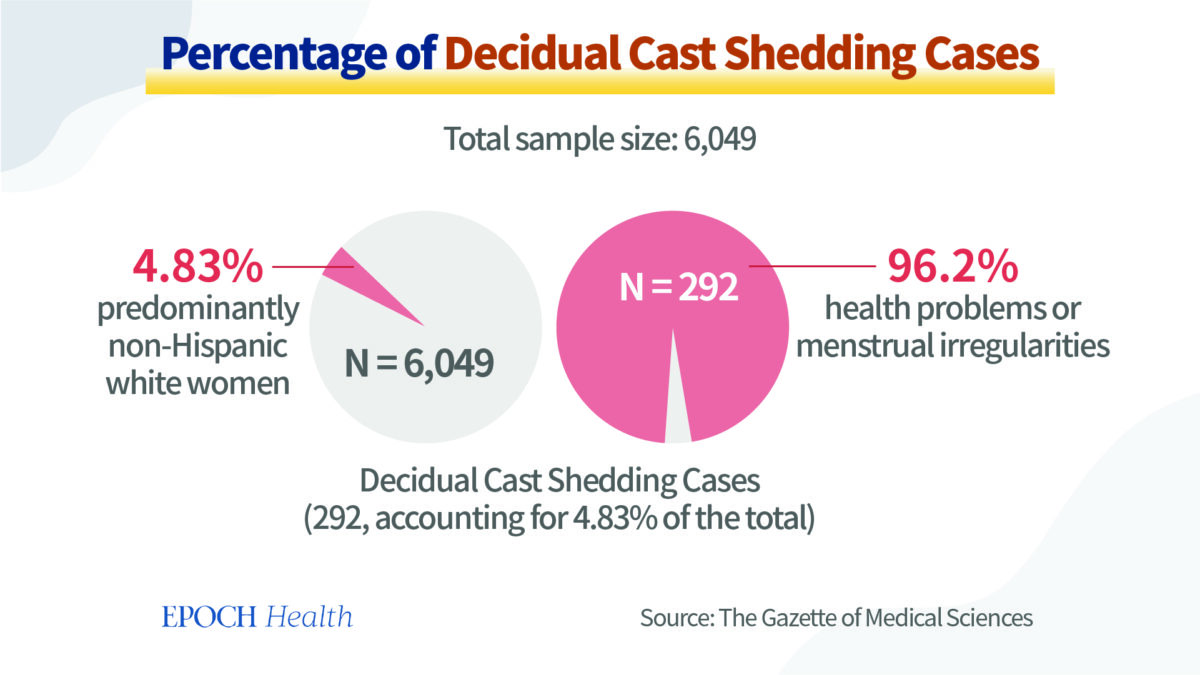
292 women reported having experienced DCS when filling out the study’s online survey, accounting for 4.83 percent of a total sample size of 6,049 survey participants. The majority of these 292 respondents were non-Hispanic Caucasian females, with a mean age of 36.1 years. Among them, 94.3 percent considered themselves healthy, and 96.2 percent started experiencing menstrual irregularities or other health issues in 2021. Specifically, 88.6 percent of these 292 respondents had regular menstrual cycles in the past, and suddenly, they started experiencing DCS, a serious yet rare condition.
At the same time, search trends on Google showed that web searches for “decidual cast shedding” increased by 2,000 percent from the first quarter of 2021 to June 2021. This also proves that there was an unprecedented increase in DCS cases in 2021, and it can still be the case in 2022, as more people received COVID-19 vaccines since the conclusion of this survey. Obviously, more research is needed to investigate the underlying causes of this sudden jump in DCS cases.
Possible Causes for Gynecological Adverse Events after COVID-19 Vaccination
So what are the possible causes of these post-vaccination gynecological and pregnancy-related adverse events?
The majority of COVID-19 vaccines are delivered with a lipid nanoparticle (LNP) formulation. After vaccination, the mRNA enters the cells and produces spike proteins by using materials within the cells. The spike proteins are supposed to trigger an immune response, which then produces neutralizing antibodies to prevent the body from being infected by the SARS-COV-2 virus.
However, according to a study published in 2021 in the journal Cell Press, LNPs are highly inflammatory. This study performed intradermal and intramuscular injections of LNPs into lab rats, which produced inflammatory cytokines and chemokines in these rats. And when intranasal injections were made, in addition to robust inflammatory responses, severe illness cases and deaths were also observed in lab rats. Furthermore, according to Pfizer’s study, after entering the human body, LNPs can travel to and accumulate in different organs, including the liver, spleen, adrenal glands, and ovaries.
As LNPs can deposit in ovaries in large quantities, they might contribute to some of the aforementioned gynecological conditions. However, the mechanisms regarding LNPs’ effects on the human body haven’t been studied in depth.
The use of LNPs, whose side effects still haven’t been thoroughly studied or comprehended, was seriously debated and still under further study before the rollout of COVID-19 vaccines. However, the emergency situation of the pandemic control measures provided health agencies and vaccine producers an unprecedented opportunity to bypass this serious issue. Was this merely an oversight?
To date, there have been few reported cases of injury from the COVID-19 vaccines in the mainstream media. However, there are still many sources of information that are available to show that the vaccines can potentially cause harm to humans. These sources include independent studies such as the aforementioned MyCycleStory.com, some concerned physicians such as Dr. Peter McCullough, Dr. Daniel Nagase, and Dr. Theresa Long (a flight surgeon who specially trained in the U.S. Defense Military Epidemiological Database [DMED], some adverse event tracking organizations (e.g. the UK government’s Yellow Card reporting on the safety issues of the COVID-19 vaccines, the European Medicines Agency’s [EMA] EudraVigilance system, the WHO’s VigiAccess, and the CDC’s Vaccine Adverse Event Reporting System [VAERS]), as well as vaccine producers’ own reports (e.g. Pfizer 5.3.6 post-marketing analysis).
Recommendations to Global Policy Makers
As the subsequent repercussions of the COVID-19 vaccination have far exceeded people’s previous expectations, the authorities should look into pausing the vaccines’ implementation, until more investigations and research are conducted on their side effects and potential risks.
Although, as aforementioned, miscarriage is one type of adverse effect after COVID-19 vaccination, so far, no government or health authorities have launched any investigations into claims of miscarriage due to vaccination. And even if the vaccine producers have been conducting such investigations into their own products, it would be merely part of their post-marketing surveillance. Such surveillance’s degree of rigorousness depends entirely on these pharmaceutical companies’ own standards, as the supervisory capacity of the regulatory authorities is even more limited in this area.
Given all the facts and potential risks regarding COVID-19 vaccines, physicians and national policymakers should take a conservative approach in recommending COVID-19 vaccines to pregnant mothers and women with underlying gynecological diseases.
Previously, some vaccines with less severe adverse effects than those of COVID-19 vaccines have been halted, including the 1976 swine flu vaccine that was removed from the market after over 25 reported deaths (according to some sources, the estimated number of deaths was 32) and the 1998 rotavirus vaccine that was removed due to a small number of non-fatal intussusception cases.
Currently, the World Council for Health recommends the halting of COVID-19 vaccine use in pregnancy until long-term safety data become available. However, the CDC and the UK’s National Health Service (NHS) still strongly recommend pregnant mothers get vaccinated against COVID-19.
Some of the previous assumptions about the SARS-CoV-2 virus at the beginning of the COVID-19 pandemic were erroneous. For instance, it was previously thought that pregnant women are at a greater risk for complications of COVID-19 infections. However, according to a large-scale study published in 2021 in the Annals of Internal Medicine, the examination of a cohort consisting of 1,062 pregnant and 9,815 nonpregnant patients hospitalized with the COVID-19 infection or viral pneumonia showed that the in-hospital death rate among pregnant patients and nonpregnant patients were 0.8 percent and 3.5 percent respectively. Thus, pregnant patients were less like to die than nonpregnant patients. Possible reasons might be that the pregnant patients were generally younger than nonpregnant ones. Additionally, pregnant patients were also less likely to have hypertension, diabetes, chronic pulmonary disease, or other comorbid conditions.
Furthermore, the use of vitamins, supplements, and some repurposed drugs, like Ivermectin, are safe and effective in treating COVID-19 infections.
Therefore, national legislators of health policies should consider the conservative approach of not recommending COVID-19 vaccination to pregnant individuals, until reliable long-term safety data become available. It is time to halt the recommendation of COVID-19 vaccines, including all the booster shots, to pregnant women. The medical field and health agencies should still adhere to the fundamental ethical principle of “Do No Harms.”
Views expressed in this article are the opinions of the author and do not necessarily reflect the views of The Epoch Times. Epoch Health welcomes professional discussion and friendly debate. To submit an opinion piece, please follow these guidelines and submit through our form here.