
A 52-year-old patient was newly committed to getting healthy—walking daily, eating better, and feeling strong—when a sharp pain flared in her chest. She assumed that it was a pulled muscle, and subsequent tests looked normal. Still, her doctor ordered a cardiac CT scan “just to be safe,” Dr. Rita Redberg, a cardiologist at the University of California–San Francisco, recounted to The Epoch Times.
The patient’s CT scan revealed no clear abnormalities. However, her doctor then ordered a follow-up catheterization that tore a major artery, forcing emergency surgery. Within months, she’d undergone bypass surgery, followed by more complications and, finally, a heart transplant.
“She was perfectly normal when she walked in [to her doctor’s office],” Redberg said. “All this [happened] because a doctor ordered a test that shouldn’t have been ordered.”
First described in Archives of Internal Medicine and later cited in Redberg’s “Less Is More” series, the case has become a parable of the medical cascade, or when one well-intentioned test can set off a chain of harm. Variations of this story unfold every day in exam rooms and hospitals across the country.
How a Medical Cascade Begins
A “cascade” doesn’t always start with a crisis. More often, it begins with something routine: an antibiotic, an X-ray order, or a precaution.
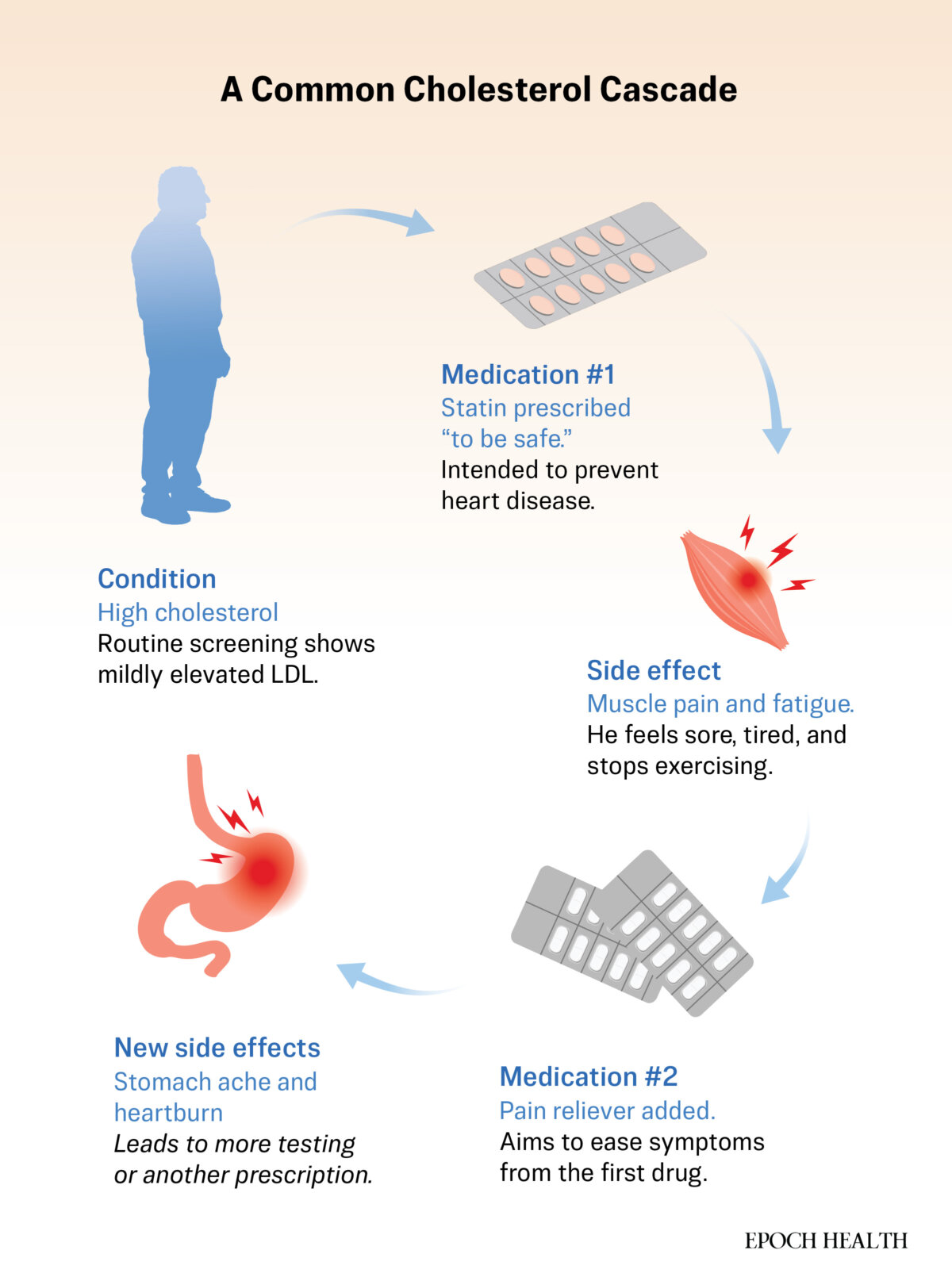
For instance, a patient may take antibiotics for a sinus infection, which clears up, but the drug may have unsettled her gut. Diarrhea could turn to bloating, with another drug prescribed to ease the side effects. Within weeks, the patient could be receiving treatments for the side effects of the medicine, rather than the illness itself. Researchers call this scenario a prescribing cascade.
A 2022 review found that such chains are a leading cause of polypharmacy, or patients taking multiple drugs at once. A 2023 study of more than 7 million people identified 49 distinct cascade pathways, many of which were triggered by cardiovascular drugs. Older adults were hit hardest.
The same spiral can begin after a scan, even when nothing is technically “wrong.”
In a 2019 national survey, nearly every U.S. physician reported seeing cascades triggered by incidental findings: small nodules, borderline measurements, or anatomical quirks discovered while looking for something else entirely.
A CT scan ordered for back pain reveals a tiny lung nodule. An MRI for headaches shows a benign cyst. The finding is described as “probably nothing,” but it rarely ends there. Another scan is scheduled. A referral follows. Sometimes, a biopsy follows.
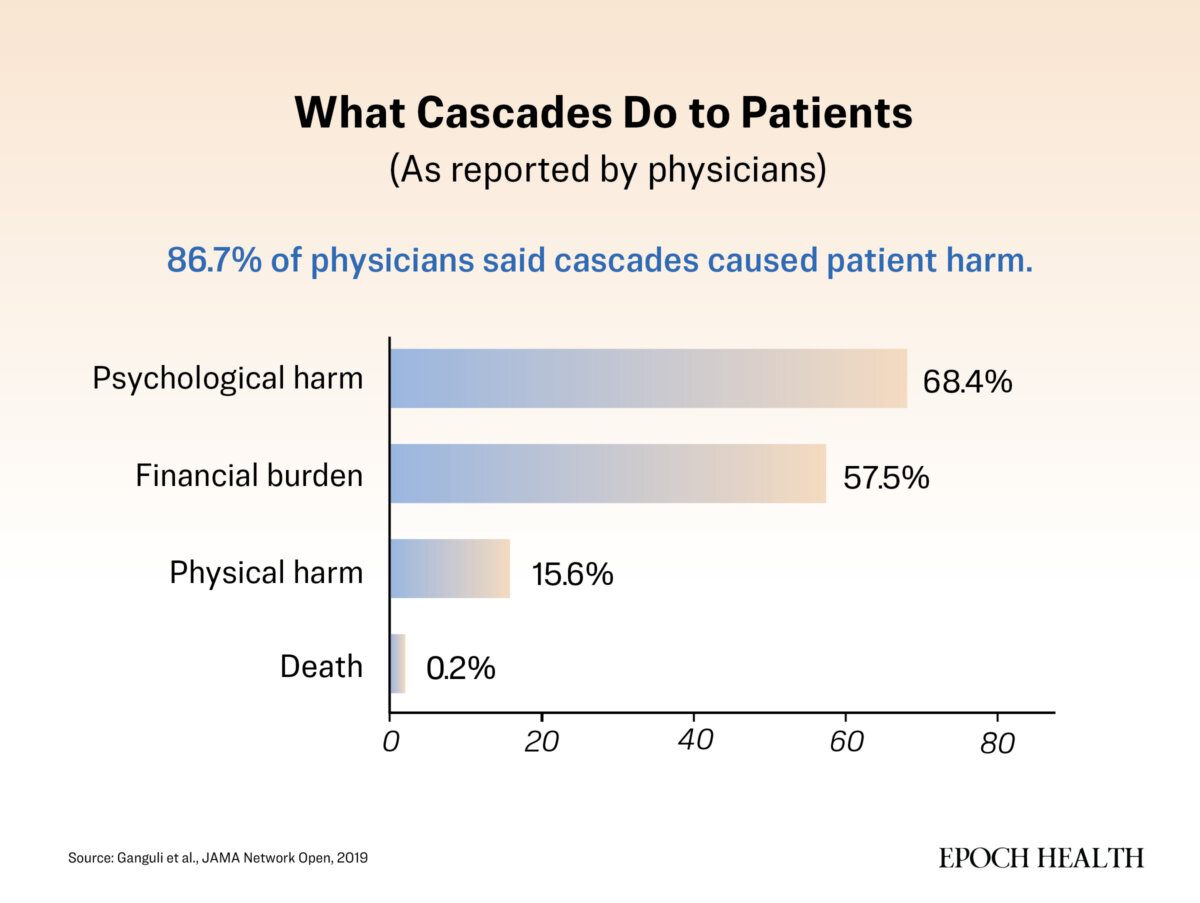
Most physicians surveyed said these findings added little or no clinical benefit, but they still set off chains of follow-up testing, anxiety, and, in some cases, harm.
“Families want 12 specialists, tons of medicine—they just want to fix every little thing,” Dr. Andy Lazris, a geriatrician and coauthor of “A Return to Healing,” told The Epoch Times. “They don’t realize how dangerous that can be, especially as the body gets older.”
What appears to be thorough care can quietly pull everyone off course. Each step feels sensible in the moment. Only later does the pattern reveal itself. The chain is built from caution, not carelessness.
Why Cascades Happen
Most cascades begin with uncertainty and our discomfort with it.
In earlier reporting, we examined cases in which symptoms persisted despite “normal” test results, when more clarity was warranted. Cascades arise when that impulse flips: When tests uncover findings that don’t explain symptoms but that still feel too unsettling to leave alone.
Imaging often fuels that chase. A 2024 global review estimated that of the more than 3.6 billion scans performed each year, up to half add little clinical value. The waste runs into billions of dollars, but the deeper cost is what follows: more procedures, more anxiety, and harm disguised as diligence.
Lazris said much of modern excess begins long before the test itself—not with recognizing decline, but with how medicine responds to it.
“We’ve created epidemics out of numbers,” he said. “Every time thresholds shift—blood pressure, diabetes, bone density—we label more people as sick and reach for a medical fix.”
Once a label appears, medicine’s instinct is to act.
“Even when there is nothing we can do that will lengthen life or improve quality of life, there seems to be a big incentive to do something anyway,” Redberg said.
The problem, both doctors said, is not failing to notice early signs of change, but mistaking medical intervention for the only—or best—response.
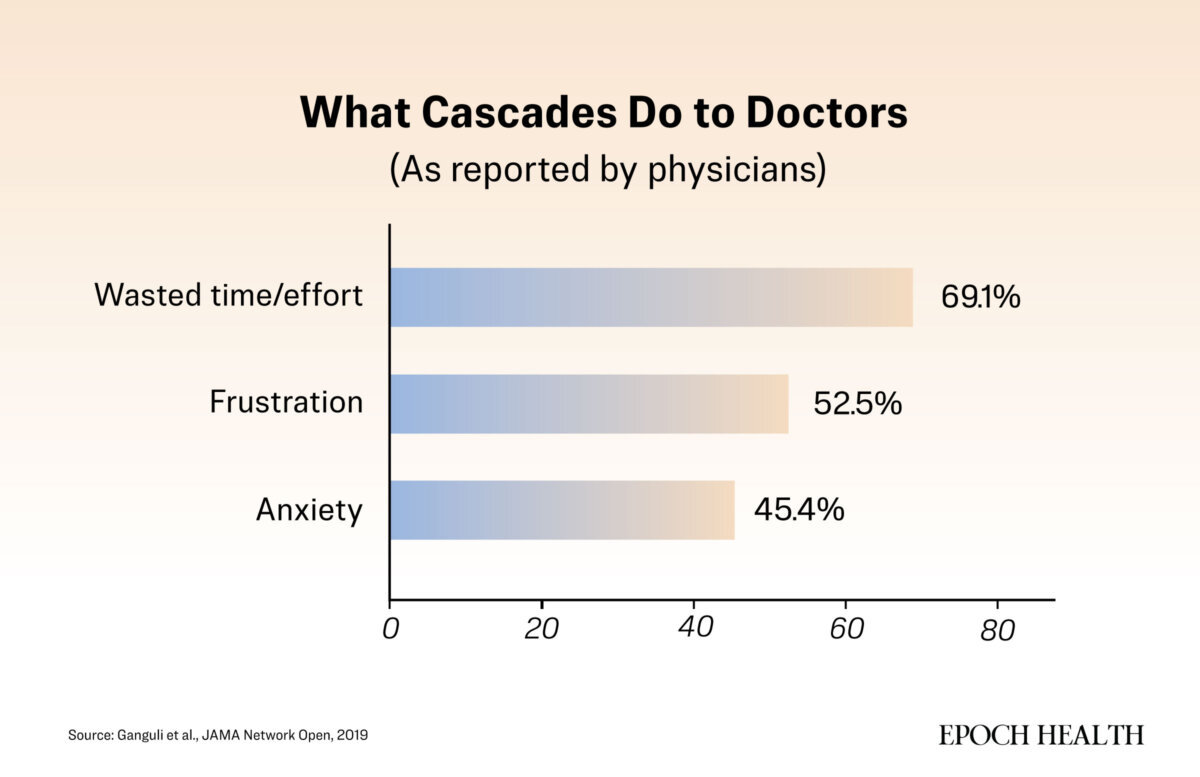
That impulse runs deep, and it is also structural. Nearly all the physicians in the 2019 national survey said they had been drawn into cascades that began with an unexpected result. Most findings proved harmless, but the process rarely stopped there. Once a test reveals something, it’s hard not to keep looking.
In the United States, physicians are often compensated based on the volume of services provided, rather than the outcomes achieved.
“We get paid for doing things,” Redberg said. “It’s hard to think that doesn’t shape the culture, even unconsciously.”
Yet money isn’t the only driver.
“It’s a reactive system,” Dr. Todd LePine, who is board-certified in internal medicine with four decades of experience, told The Epoch Times. Doing something feels like progress, but sometimes waiting would serve the patient better.
Redberg sees the same psychology on both sides of the exam table.
“We’ve confused care with intervention,” she said. Patients share that reflex.
“I’ll ask how they’re feeling, and they’ll say, ‘You tell me, Dr. Redberg,'” she said. “They’ve learned to equate health with test results.”
Between doctors eager to help and patients expecting action, medicine can trap itself in motion. Reassurance comes from another scan, not a conversation. However, according to Redberg, “People aren’t reassured by tests.”
“They’re reassured by someone who listens,” she said.
For patients navigating a system built on intervention, it’s not always easy to see when good care begins to go off course.
Spotting When Care Starts to Spiral
Cascades rarely look reckless as they unfold. Each step feels reasonable, even careful. But when treatment starts drifting from its purpose, it’s time to take stock. Here are some common signals.
The Original Problem Is Gone, but Monitoring Continues
Scenario: You went in for a sinus infection or a muscle strain. It resolved, but follow-up imaging, labs, or check-ins continue, even though your symptoms are gone.
What to Ask: What problem are we still monitoring, and what would change if we stopped?
Test Numbers Look Better, but You Feel Worse
Scenario: Your labs have improved, but your energy or mood has declined.
What to Ask: Are the numbers driving my treatment, or is how I’m actually doing driving it?
A Test Leads to More Tests Rather Than Answers
Scenario: A scan finds something “incidental.” You’re told that it’s probably nothing, but another scan is ordered, then a specialist visit.
What to Ask: What are we hoping to find, and what would we do with that information?
You Are Told, ‘Just to Be Safe’
Scenario: Hearing about extra caution sounds comforting, but it often signals action driven by uncertainty rather than evidence.
What to Ask: What are the risks of doing nothing right now?
Your List of Medications Is Growing
Scenario: You’re on more than five drugs.
What to Ask: Which drug can we taper first, and how will we know that it’s safe to do so?
You’re Treating Medication Side Effects, Not Illness
Scenario: A medication causes fatigue, dizziness, or stomach issues. Another drug is added to manage that side effect, then another to manage the next.
What to Ask: Can we reduce or stop the original medication instead of adding another?
The Plan No Longer Matches the Original Concern
Scenario: After months of tests, referrals, or medications, the current plan feels disconnected from why you sought care in the first place.
What to Ask: What is the main goal of my treatment right now, and does it still match my original concern?
Not every cascade is harmful. Some interventions are necessary and even life-saving. However, knowing when care has drifted from your true goal is the first step in regaining control.
When to Hit Pause
Every test should have a plan for what to do with the result, and sometimes, the right plan is to do nothing, according to Redberg.
That idea runs counter to how most of us think about health care. We’re taught to fix, intervene, and keep moving. But medicine doesn’t always reward speed.
“Time itself is in your favor,” Lazris said. “Especially in older adults—going slow is crucial.” A brief period of watchful waiting, accompanied by a clear follow-up plan, can help distinguish between problems that resolve on their own and those that require care.
Slowing down is not about withholding care; it is about resisting reflex. The same tools that save lives can also start a chain reaction when used without a clear purpose. Knowing when to wait or stop takes judgment and trust.
Helping doesn’t always mean acting, according to Redberg.
“Sometimes talking and reassuring are the most important things we do,” she said.
What’s Next: Slowing down medicine is only part of being a wise patient. The next step is knowing when to begin, especially with the screenings meant to keep us healthy. Our next article explores what to ask before saying “yes” to routine tests and how to balance prevention with the risks of overdiagnosis.