
When Jennifer’s doctor asked about her last MRI, she paused. She knew the results were somewhere—an email, an online patient portal, maybe a CD from a hospital she no longer used—but she couldn’t remember the date or where to look. With no time to search, the visit moved on.
It’s a familiar moment in American exam rooms. As care spreads across specialists, hospitals, and health systems, medical records scatter with it. Many patients now receive care across multiple systems, often juggling two, three, or more portals that don’t communicate with one another.
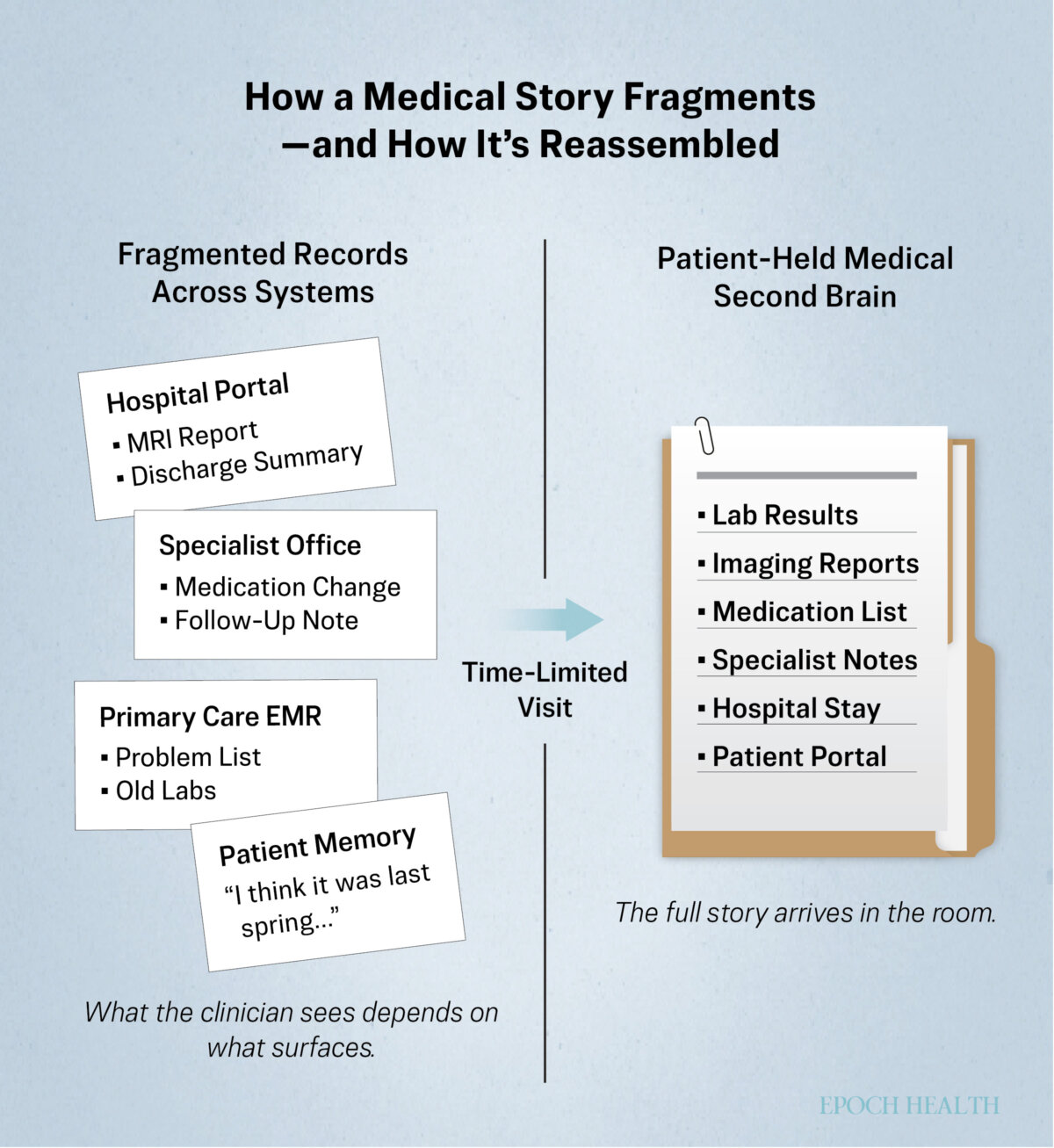
As records fragment, the task of holding our health stories together increasingly falls to the patient. When key details are missing or hard to retrieve, diagnosis doesn’t pause. Clinicians move forward with whatever information surfaces first.
The emerging situation has turned record-keeping into more than a clerical task. It has become key to getting effective care and a way for patients to preserve context across visits, specialists, and years of care.
That’s where a medical “second brain” comes in. It’s a personal system for keeping essential health information—diagnoses, medications, test results, and care history—in one place, under the patient’s control. It doesn’t fix a fragmented health care system, but it can steady a patient’s experience by keeping critical details visible when decisions need to be made.
Why Do You Need a Medical Second Brain?
As doctor visits grow shorter and their patient loads heavier, their ability to reconstruct a patient’s history has withered. Clinicians may be attentive, but time is limited.
A portable medical record, or a medical second brain, is designed for that reality. Whether digital or on paper, it keeps essential details at hand when memory, portals, or time fall short.
The risks of missing information are well documented. Research on diagnostic error shows that incomplete or inaccessible records can delay diagnosis and lead to unnecessary testing. A 2015 report from the National Academies of Sciences, Engineering, and Medicine identified poor information flow and fragmented records as major threats to patient safety, especially during transitions between clinicians and care settings.
There’s evidence that patient-held records can help close those gaps. In a randomized trial published in BMJ Global Health, clinicians were significantly more likely to have essential information available when patients carried a portable health record, reducing time spent reconstructing history and frustration on both sides of the visit.
Availability can change how an encounter unfolds. When patients can clearly summarize their history or share key results, visits tend to move faster, and decisions come into focus.
Even then, critical context can be missed. That becomes even more likely when the system feels data-rich. Records may appear complete while containing errors, outdated information, or missing critical details. Even a polished medical history can be misleading if key facts are missing or wrong.
“Getting the correct diagnosis is entirely dependent on getting all the facts on the table, and they better be the correct facts,” Dr. Mark Graber, a professor emeritus of medicine at Stony Brook University and the founder of Community Improving Diagnosis in Medicine, told The Epoch Times in an email. “Just change a thing or two, like which symptoms are the most important ones, and the whole differential diagnosis changes.”
Why Patient Portals Aren’t Enough
Most people now have access to an online portal such as MyChart. These tools can be genuinely useful, offering test results, visit notes, and messaging. For care delivered within a single health system, they often work as intended.
The problem is that patient portals are built around institutions rather than continuity. Each health system maintains its own record, organized by encounters, departments, and billing events—reflecting how care is delivered and documented inside the system, not how illness unfolds over time.
As a result, portals preserve data but not narrative. A lab result may appear, but why it was ordered, how it compares to prior results elsewhere, or what changed afterward may live in a different visit, a different system—or nowhere at all.
Portals also fragment time. When patients change doctors, move, switch insurers, or see specialists across systems, their history splinters into parallel timelines. What looks complete inside one portal is often only a slice of a much longer story.
“Patients assume ‘it’s all in there’ and that the doctors either know it or can find it,” Graber said. “In fact, the important things may or may not be in there, and their doctors or team may or may not be able to find it.”
Even within a single system, accuracy isn’t guaranteed.
“The EMR [electronic medical record] is a mess and often inaccurate,” Graber said, referring to the way records accumulate errors, outdated details, and copied-forward notes over time.
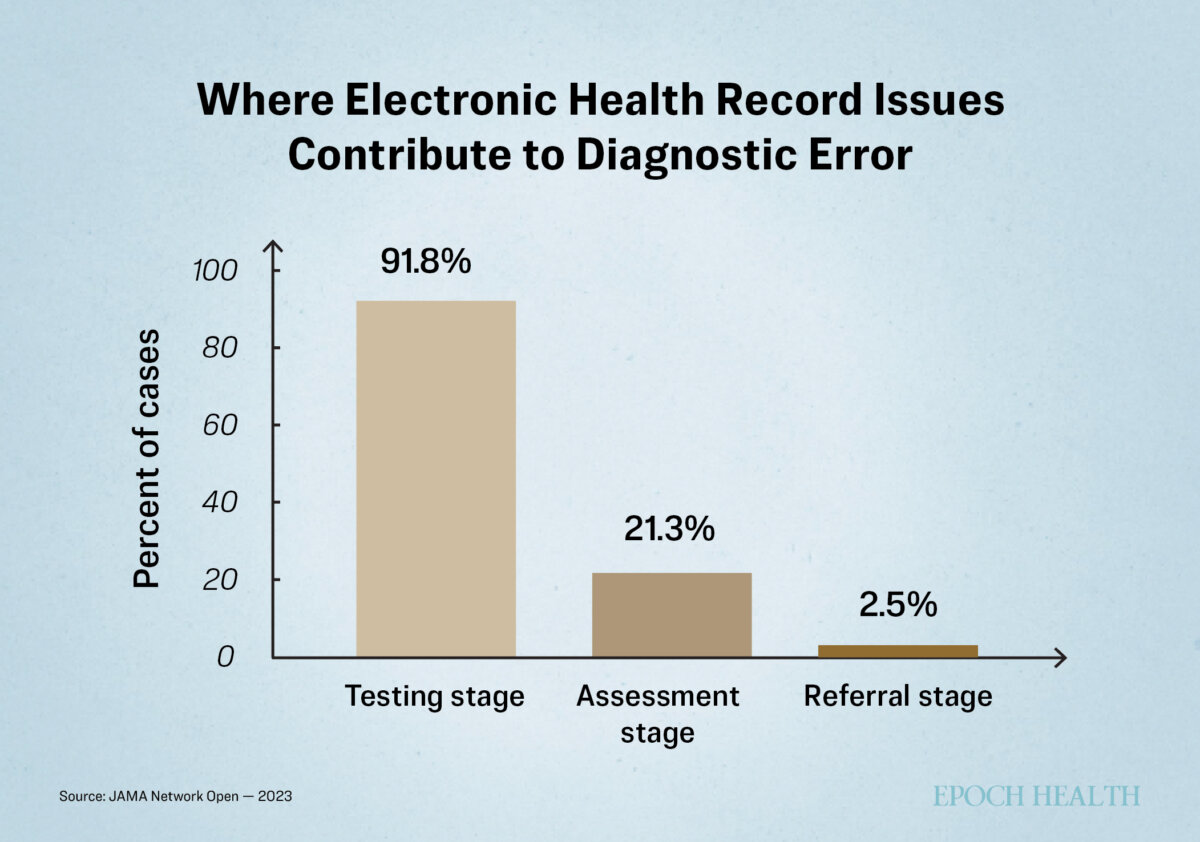
Research bears that out. In a 2023 analysis of closed malpractice claims, published in JAMA Network Open, electronic health record issues were identified as a potential contributor to diagnostic errors in about 61 percent of cases, most commonly when test results and related information failed to surface during visits.
Health record mismatch quietly shifts the burden of continuity to patients. They are expected to remember, reconcile, and reiterate their history—and to know their record well enough to catch errors when they arise.
A medical second brain makes this task possible. It doesn’t replace patient portals—it pulls from them.
Most portals allow patients to download key documents as PDFs, which can then be stored alongside records from other systems. Used this way, portals become sources rather than the whole record. The second brain becomes the place where the story is reassembled across institutions and over time in a form that can actually be carried into the medical office.

What to Include in Your Medical Second Brain
A medical second brain works best when it’s selective. The goal isn’t to recreate your full medical record but to make the most decision-shaping information easy to find when it’s needed.
The principle aligns with guidance from patient-safety researchers and academic medical centers, which consistently emphasize summary, clarity, and recency over volume. Johns Hopkins Medicine advises patients to treat portable medical records as they would a resume, identifying a health goal and returning to it again and again.
Clinicians tend to look for information in layers. They start with what affects decisions now, then widen the frame only if needed. Start with what matters most, then build outward.
A Current Health Snapshot
Your current health snapshot is the foundation. Many hospitals recommend that patients keep an updated list of active conditions and medications that can be quickly shared during visits or emergencies.
Include:
- Active diagnoses or conditions
- Current medications, with doses and schedules
- Supplements that could affect care
- Known allergies or adverse reactions
- Implanted devices or medical hardware
Kept to a page, this snapshot helps orient the visit before time runs out.
Recent Results That Shape Decisions
Not every test belongs in “recent results”—only the ones that currently influence care.
Include:
- Key lab results from the past few years
- Imaging reports that are still clinically relevant
- Pathology reports tied to ongoing conditions
Keep summaries or impressions upfront. Full reports can live behind them, clearly labeled and dated.
Major Medical History
A major medical history provides context without overwhelming detail.
Include
- Relevant surgeries
- Hospitalizations
- Chronic illnesses
- Significant injuries
Dates matter more than narrative. A short timeline is often enough.
Care Team and Points of Contact
When records don’t move cleanly between systems, patients often become the only reliable link between their clinicians.
Keeping a current list of clinicians, their roles, and contact information can prevent delays when coordination is needed, particularly during referrals or emergencies.
Insurance and Planning Documents
Insurance and planning documents are rarely needed—until they are.
Include a copy of your insurance card, along with any advance directive or health care proxy—documents that guide care when you may not be able to speak for yourself. These will be covered in greater depth in the next article. Keep this section clearly marked and easy to share if necessary.
How to Build a Medical Second Brain
You don’t need special software or a weekend set aside. Most medical second brains come together gradually, test by test, visit by visit.
Many patients discover, through trial and error, that the most sustainable systems are layered. A full archive of medical records may exist for insurance or record-keeping, while a slimmer, up-to-date set stays ready for actual visits. The second brain focuses only on what currently shapes care, keeping the rest out of the way.
Choose a Format You’ll Actually Use
Start with what fits your habits.
Some people prefer a digital folder that they can search and share easily. Others feel more comfortable with a paper binder or accordion file that they can flip through in an exam room. Many use both: a digital version for storage and sharing and a slim paper summary for appointments.
The best system is the one you will keep up.
Gather What Already Exists
Much of what you need is already available, just scattered.
Download records from patient portals. Request copies of recent labs, imaging reports, and discharge summaries. If you have had imaging done elsewhere, request a digital copy you can store yourself.
Focus first on the past few years and on conditions that currently shape your care. For clinicians, missing information narrows decisions. When time is short, care defaults to what’s immediately visible. A medical second brain helps ensure that important context doesn’t fall out of the conversation simply because it lives in another system or another year.
Organize for Speed, Not Perfection
Group documents by type, then order them by date, with the most recent on top. Clear labels matter more than exhaustive filing. A folder called “Labs—Recent” is more useful than one divided into subcategories that no one has time to navigate.
If you’re using digital files, consistent naming helps—dates first, then the test or visit, then the provider.
Add Context in Your Own Words
Providing a personal narrative is one step patients often skip—and the one clinicians find most helpful.
After a visit, jot down what changed: a new diagnosis, a medication adjustment, a plan to watch and wait. A few sentences can save minutes of reconstruction later.
Over time, your notes become a running explanation of how your care has evolved.
Keep It Lightly Maintained
A medical second brain works best as a living document, not a project you finish.
Update it after visits. Review it occasionally to remove duplicates and outdated medications. If something no longer matters, let it go.
Many people worry that they’re doing the document wrong. In practice, there is no single correct system. A medical second brain only needs to be good enough to help you orient, ask better questions, and avoid starting from scratch. It can be messy, partial, and still work.
For some people, what works includes a stripped-down version on their phone—current medications, allergies, diagnoses, and emergency contacts—available when there’s no time to explain.
[series_posts_list][/series_posts_list]
How to Use Your Medical Second Brain
A medical second brain matters most at times of change—a new diagnosis, a medication adjustment, or a test result that raises new questions.
Capturing what changed—and why—helps preserve context that often fades once the visit ends and care moves on.
It’s just as useful when progress slows. Delays are easier to spot when patients track what’s been ordered, what’s pending, and what needs follow-up, especially when no single clinician is overseeing the full plan.
Tracking changes becomes essential when care crosses boundaries: a referral to a new specialist, a second opinion, or a move between health systems. Rather than reconstructing your history from memory, you can share it in its entirety from your records.
Those moments are particularly vulnerable, according to Graber.
“These summaries would be so helpful, critical in instances where one practice or hospital does not share the EMR from a patient’s prior care settings,” he said.
You will not need your medical second brain every day. But when decisions accelerate or continuity is at risk, having your own records can stabilize care. In a health care system built in pieces, it’s one way to keep your story whole.
You don’t need to manage the system. You just need a single place where your story doesn’t get lost.
What’s Next: Keeping your medical story organized helps guide decisions in the moment. Next, we turn to the essential medical paperwork that makes sure your wishes are honored when you can’t speak for yourself.