

Stacy Smith lived two different lives: professional, church-going girl in public and laid-back, pot-smoking girl in private. The ruse was exhausting.
“Marijuana was running the show. I knew it was an addiction,” the 47-year-old mother of five told The Epoch Times.
Yet Smith rationalized that it wasn’t meth or heroin, and she was functioning and responsible.
As cravings intensified, she began closing herself off from her children to smoke, turning down church gatherings, afraid she’d be judged and rejected if they smelled marijuana on her clothes.
“I realized it was something I ran to before I ran to God,” she said. “I wanted to quit because I knew it had become my god.”
Smith’s story reflects a growing crisis that’s reshaping America’s relationship with marijuana: An estimated 19 million Americans aged 12 and older now battle cannabis addiction—about 30 percent of all users, according to the 2023 U.S. National Survey on Drug Use and Health.
Evidence connects addiction to higher potency products and recreational use of cannabis, especially beginning in adolescence.
President Donald Trump recently signed an executive order to reclassify marijuana as a Schedule III drug, a decision viewed as acknowledging that it may have some accepted medical use while still recognizing its high potential for abuse and dependence. The move comes as researchers, doctors, and patients grapple with products that bear little resemblance to the marijuana of previous generations.
How Marijuana Has Changed
“People have been touting that marijuana is not addicting, which is absolutely false,” addiction psychiatrist Dr. Elizabeth Stuyt told The Epoch Times. “Old-time cannabis probably wasn’t very addicting, but you can’t even find that anymore.”
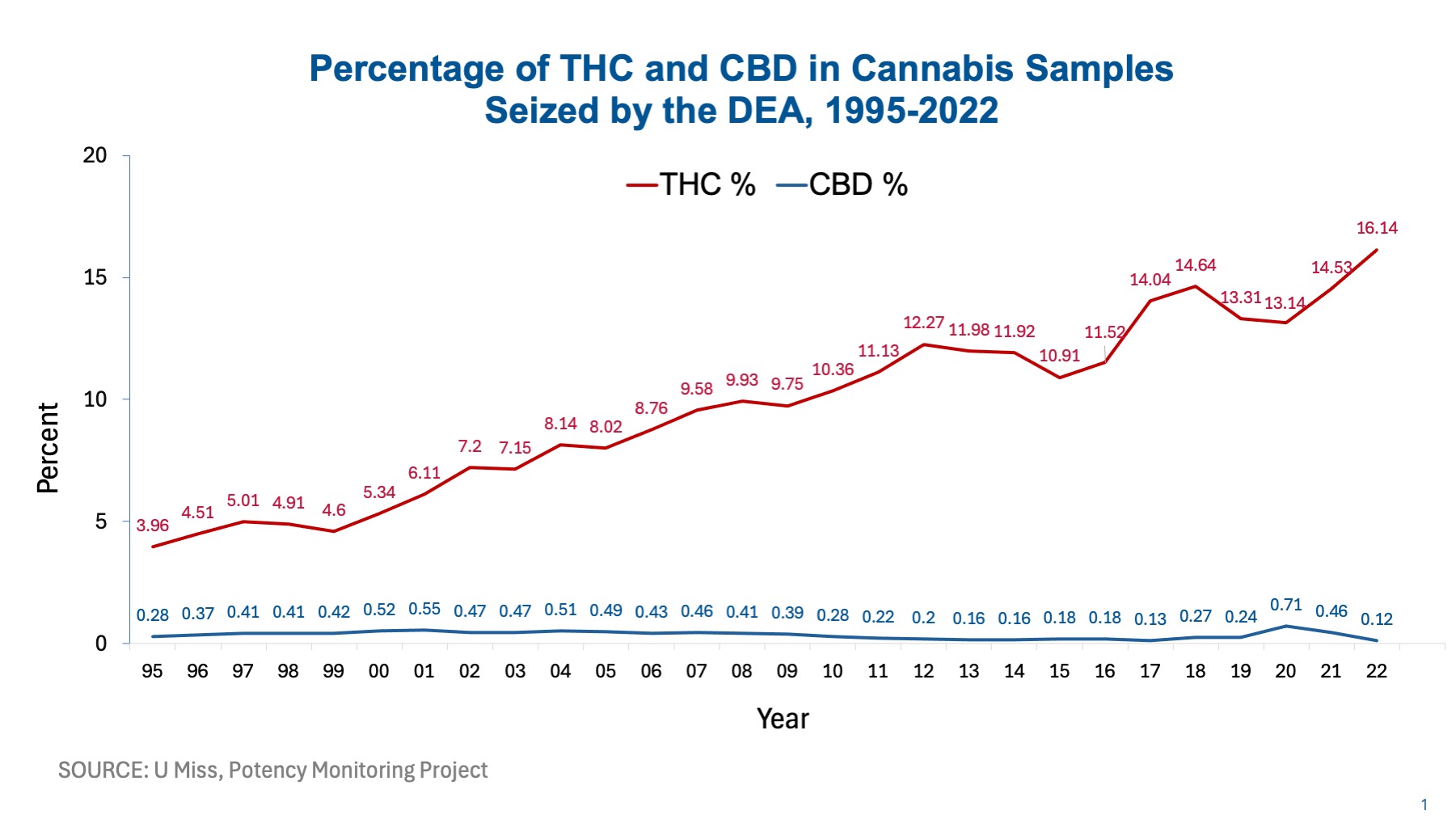
The chemistry tells the story. Cannabis samples seized by the U.S. Drug Enforcement Agency in 1995 contained less than 5 percent tetrahydrocannabinol (THC)—the psychoactive compound that produces a “high.” In 2022, seized samples had more than 16 percent THC. Products sold in legal markets at licensed dispensaries reflect the same trend, according to a study in Frontiers in Pharmacology.
{kind=link}
Not only do plants contain more THC, but also, both medicinal and non-medicinal products on the market often contain higher percentages of THC. A systematic review published in the American Journal of Psychiatry noted a continuum of potency for smokable cannabis in which less than 10 percent THC was considered low and above 20 percent was classified as high.
“These really high-THC products have produced some pretty significant addiction,” Stuyt said.
She noted that some professionals describe it as THC addiction rather than cannabis addiction to distinguish modern products from those of older generations.
The problem extends beyond potency. While THC levels have tripled, levels of cannabidiol (CBD)—the compound that helps lower inflammation, pain, and anxiety—have remained stable in seized marijuana samples. A balanced THC to CBD ratio of one to one is commonly suggested in clinical studies as being most beneficial for symptom relief while offsetting the adverse effects of THC, although evidence is mixed.
The problem is that although THC potency is heavily marketed in dispensary products, consumers may be at risk of unwanted side effects from unbalanced cannabis products and not even know it. One study published in Frontiers in Pharmacology found that more than half of the products assessed in nine states had no information on CBD content.
Once the levels and ratios were assessed, most products were found to be highly intoxicating because of unbalanced ratios and only suitable for users who have built up tolerance. A small number of the products were acceptable therapeutic options.
“This study’s results are alarming,” the authors wrote. “Combined with holes in popular knowledge and misconceptions about THC and CBD, the current market can lead to problematic patient dosing as they try to maximize therapeutic benefits, such as analgesia, while subjecting themselves to THC’s acute intoxicating effects.”
When Stuyt first noted that cannabis made her patients anxious, paranoid, or dependent, she recommended products with 10 percent THC or lower. She quickly realized that such products are nearly impossible to find, even as 40 states now permit medical marijuana use.
Stuyt noted that her colleagues trying to use medicinal cannabis often recommend a patchwork of products in order to find the right ratio.
The Paradoxes
High-potency cannabis, especially products with much more THC than CBD, could explain cannabis addiction and increasing rates of conditions linked to cannabis use.
Among the most difficult disorders for users to deal with, Stuyt said, is cannabinoid hyperemesis syndrome, a severe cyclical vomiting disorder.
“It is such a hard sell to convince people that cannabis is causing their symptoms—they just can’t believe it because it’s supposed to help with nausea and vomiting,” she said.
Cannabis users seeking relaxation face another paradox. Often gravitating to it for its relaxing effect, cannabis users are at higher risk of psychosis, Dr. Nora D. Volkow, a leading addiction researcher and director of the National Institute on Drug Abuse, told The Epoch Times.
In some cases, it can lead to chronic, disruptive psychotic disorders such as schizophrenia and delusional disorder. Research has shown that the increased risk of psychosis for those who use cannabis most frequently is between 50 percent and 200 percent. The drug can also cause intoxication-related anxiety and social withdrawal—the very symptoms users often hope to alleviate.
Suicidal ideation is also linked to cannabis use, which Volkow called concerning, even though research hasn’t determined whether the relationship is because those with higher suicidal ideation are drawn to cannabis use as a means of coping.
The expected anti-nausea effects of marijuana also make it a common drug of choice for pregnant women suffering from morning sickness, Volkow said. However, a mother’s use of cannabis can affect her child’s overall brain size and put the child at risk of brain changes associated with attention-deficit/hyperactivity disorder and mild psychotic symptoms.
Although cannabis doesn’t cause fatal outcomes like opioid overdoses do, she said, it can indirectly cause death from accidents when someone has become intoxicated or from strokes and heart attacks triggered by very high THC levels.
“The reality is that cannabis has some really serious negative effects, particularly for some people, and we don’t know who is most vulnerable,” she said.
What Helps
Family and friends of cannabis users can be critical for assessing potential use disorders, Volkow said, because self-diagnosis is rare.
“We always have that tendency to explain our behaviors, and it’s very difficult to admit that something is wrong,” she said. “The fact that cannabis may be less addictive than other drugs like cocaine or methamphetamine or heroin, of course, does not in and of itself deny its addictiveness.”
Common symptoms include cravings, skipping important activities to use cannabis, taking more of it or using it longer than intended, unsuccessful attempts to quit, withdrawal symptoms, and psychological, interpersonal, or physical problems. One litmus test is to quit using cannabis, she said, and note how you feel after the first few days. Withdrawal symptoms typically begin within a day, peak at the third day, and wane after two weeks. Irritability, anxiety, and insomnia can burden one to the point of relapse as a means of escaping the discomfort.
Cannabis withdrawal treatment options have little research backing or are borrowed from other addiction research, leaving those affected to cobble together questionable support or attempt quitting cold turkey.
“There’s a lot of research out there showing that people with marijuana or cannabis use disorder don’t do well in treatment, and I think that’s because they’re so uncomfortable,” Stuyt said. “They just can’t quit, and there’s nothing to help them with that, pharmaceutically.”
Gabapentin
The most promising medication currently available is gabapentin, an anti-convulsant drug used for nerve pain, Stuyt said.
In a study published in Neuropsychopharmacology, patients taking gabapentin had fewer depression symptoms and were able to stop using cannabis at a higher rate than those taking a placebo. It also outperformed the placebo for withdrawal symptoms.
Exercise
Physical activity improved the quitting rate in substance abuse disorders and also eased withdrawal, anxiety, and depression symptoms, as noted in a meta-analysis published in PLoS One.
Volkow explained the dual mechanism: New routines can replace unwanted habits, and exercise strengthens the reward and reinforcing mechanisms in the brain that have become disrupted by cannabis use, such as dopamine deficits that are a hallmark of addiction.
A study published in Neuropsychopharmacology of 19 people who were addicted to methamphetamine showed a 15 percent increase in dopamine receptors when they walked or jogged and did resistance training during treatment.
Auriculotherapy
Stuyt advocates a five-point auricular (ear) acupuncture protocol for treating withdrawal symptoms during detoxification. Despite her initial reluctance, she has helped change laws in several states to allow health care workers to obtain certification in traditional Chinese medicine procedures, thereby expanding its availability.
“Most exciting to me is that it really does help with cannabinoid hyperemesis syndrome,” she said. “When people are really sick, throwing up all the time, this really helps calm it down.”
The first pressure point used in the protocol is the sympathetic point, which helps soothe anxiety or, in traditional Chinese medicine, balance yin and yang. Stuyt noted that the point is often used in traditional acupuncture to stabilize the bowels, which might explain its effectiveness.
One systematic review published in the Journal of Addictive Diseases found that 23 of 36 studies reported that auriculotherapy was effective for treating addiction. However, the bias risk was moderate to high, the authors noted.
Behavioral Interventions
“Behavioral interventions definitely work, but it requires sustained treatment, and not everyone responds,” Volkow said.
She highlighted music therapy and other alternative behavioral interventions to support sleep and diet as promising areas of research.
Cognitive behavioral therapy, particularly when habit changes are intrinsically motivated and tied to incentives and rewards, can be helpful, she said, citing reports from patients that it works, even if research is less certain.
The authors of a meta-analysis published in Addiction exploring the effectiveness of psychosocial therapy for cannabis addiction noted that although specific forms of cognitive behavioral therapy may be more useful than doing nothing or receiving generic support, the evidence is low and uncertain.
Amino Acid Supplements
There’s also limited evidence about neuronutrient amino acids used for addiction, although amino acids are the precursors to making neurotransmitters, which are out of balance in substance abuse disorders.
Neuronutrient expert Julia Ross was first motivated to try amino acids when she was director of outpatient programs at an addiction clinic because of a study of the amino acid blend tropamine. Published in Current Therapeutic Research, the study showed that tropamine accelerated recovery for serious cocaine abusers in a 30-day hospital program.
Tropamine contains tyrosine, the precursor that naturally stimulates dopamine and norepinephrine. Her program found that, at higher doses, tyrosine relieved almost all cocaine addicts’ cravings, she said. Other amino acids raise levels of natural opiates, or endorphins, and serotonin, our natural antidepressant. Those with cannabis use disorder often need two or more of these amino acids to raise levels of various neurotransmitters affected by the drug, she said.
Spirituality
Interventions that emphasize spirituality had a moderate effect on addiction recovery in a meta-analysis published in Drug and Alcohol Dependence. The effect was statistically significant compared with other interventions, although the study focused primarily on 12-step programs because research on other spiritual and religious approaches was limited.
Breaking Free
For Smith, the turning point came at a church retreat a decade ago when she confessed her cannabis struggles to another woman, admitting her fear that she might lose some of her old friends with whom she smoked.
“I said, ‘I feel like if I quit, I’ll have no friends and I’ll be judged,’” Smith recalled. “And she was like, ‘I’ll be your friend.’ I broke down crying.”
Smith began to taper down her use, and within two months, she’d stopped. That didn’t mean there weren’t difficult moments. Not long after quitting, Smith’s husband died, and other family members gathered to grieve, bringing marijuana with them. But she resisted.
Her recovery brought greater agency, less numbness, and more disposable income. She stopped needing medicine for stomach issues and heartburn.
“It was hard for a good whole year after quitting,” she said, “but it also got easier and easier.”