
There’s a club with more than 75 million members in the United States alone, with 6,000 more joining daily. What unites them are sudden heat waves and mysterious mood shifts. This is the menopause transition—spanning perimenopause and postmenopause—a phase nearly every woman experiences in her 40s or 50s.
Menopause marks the permanent end of menstrual cycles and the close of a woman’s reproductive years. It is a natural part of aging. About 80 percent of women undergoing menopause experience unpleasant symptoms, and for many, these symptoms are severe.
Yet these symptoms can be effectively managed.
 (Illustration by The Epoch Times, Shutterstock)
(Illustration by The Epoch Times, Shutterstock)[shortcut_anchor id=”anchor_1780096802365″ label=”Stages and Symptoms”]What Are the Symptoms and Early Signs of Menopause?[/shortcut_anchor]
Menopause occurs after 12 consecutive months without a menstrual period, typically between the ages 45 and 55.
It unfolds across three stages.
Stage 1: Perimenopause
Perimenopause is the transition period before menopause, typically lasting two to 10 years, during which estrogen—a hormone that regulates the menstrual cycle—and progesterone—a hormone that prepares the uterus for pregnancy and helps regulate menstruation—levels fluctuate.
Irregular menstrual periods can be the first sign of perimenopause. They may occur more or less frequently, vary in length or flow, or even stop for months before returning.
You may experience menopause symptoms, in a milder form.
Stage 2: Menopause
Symptoms associated with menopause fall into several categories.
Vasomotor Symptoms (75 Percent to 80 Percent of Women)
Refers to the blood vessel and temperature-regulation system. These symptoms usually last one to six years, but in 10 percent of women, they can persist up to 15 years.
- Hot Flashes: They typically last from 30 seconds to 10 minutes, and can occur several times an hour or just a few times a week at unpredictable times.
- Night Sweats: Hot flashes that happen at night and can interfere with sleep.
- Heart Palpitations: Hormonal fluctuations can increase heart rate by up to 16 beats per minute, and palpitations often occur alongside hot flashes.
- Migraines: During early menopause, these hormonal changes can worsen the intensity and frequency of migraines. After menopause, most women experience an improvement.
Genitourinary Symptoms (50 Percent to 75 Percent of Women)
As estrogen declines, the vaginal lining thins and the vaginal tissue loses elasticity, leading to the following:
- Vaginal Dryness, Burning, Itching, and Irritation: These changes may also increase the risk of vaginal or urinary tract infections, as lower estrogen raises vaginal pH and allows more harmful bacteria to grow.
- Increased Urination: Caused by thinning of the urethra and sometimes accompanied by painful urination.
- Urinary Incontinence: More strongly linked to aging and other factors than menopause itself. Weakened bladder muscles can cause urine leakage when sneezing or coughing.
Musculoskeletal Symptoms (More Than 70 Percent of Women)
Lower estrogen levels can lead to bone loss (osteoporosis), making bones weaker and more likely to break. Declining estrogen also affects muscles, tendons, ligaments, cartilage, and fat.
- Joint pain, stiffness, and frozen shoulder
- Loss of lean muscle mass, increasing the risk of sarcopenia (age-related muscle loss)
- Reduced bone density, increasing the risk of osteoporosis and fractures
Psychological and Sleep Symptoms (70 Percent of Women)
Lower estrogen levels affect brain areas involved in mood and cognition, but personal life and social circumstances also play a role.
- Irritability, anxiety, and depression
- Difficulty concentrating
- Sleep problems, including insomnia, sleep apnea, and restless leg syndrome
Other Symptoms
Menopause can cause a variety of lesser-known symptoms that affect both body and mind.
- Fatigue
- Cognitive Changes: These changes often improve after menopause.
- Changes in Sexual Function
- Body Composition Changes: Reduced metabolism from declining hormones can cause increased body fat, particularly around the waist.
- Breast Tenderness
- Thinner and Drier Skin
Stage 3: Postmenopause
Postmenopause begins the day after a woman’s final menstrual period and lasts for the rest of her life. During this stage, menopausal symptoms often ease or stop, but some women continue to experience them.
Women should see a doctor if they experience vaginal bleeding after menopause, as any abnormal bleeding may indicate health issues, including endometrial, cervical, or ovarian cancers.
[shortcut_anchor id=”anchor_1780096819647″ label=”Causes”]What Causes Menopause?[/shortcut_anchor]
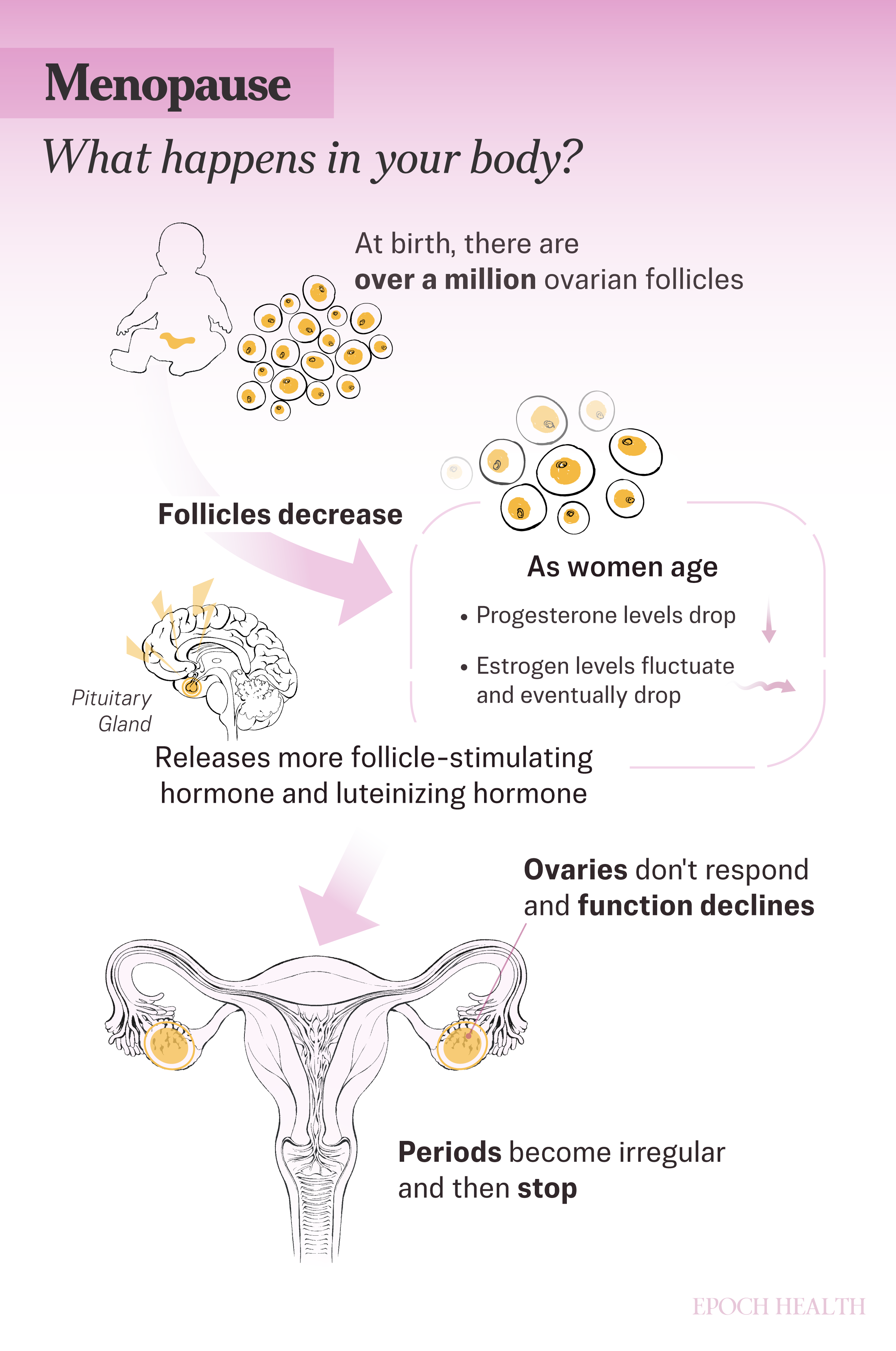
Women are born with more than one million ovarian follicles, each housing an immature egg. Over time, follicles are naturally lost or used during ovulation.
As women age, ovarian cells produce less estrogen and other hormones, such as inhibin B, which helps regulate communication between the brain and ovaries. In response to declining hormone levels, the pituitary gland releases more follicle-stimulating hormone (FSH) and luteinizing hormone (LH), in an attempt to stimulate the ovaries, but with diminishing effect.
This disruption affects communication between the brain and ovaries, changes the growth of the uterine lining, and often leads to irregular periods during the transition to menopause.
Menopause occurs when ovarian follicle reserves are depleted to the point that estrogen and progesterone production decline, ovulation stops, and menstrual periods stop completely. For most women, periods gradually stop, although occasionally the transition can be abrupt.
Menopause that occurs between ages 40 and 45 is called early menopause and happens naturally in about 5 percent of women. Certain factors can influence the timing of premature or early menopause, including the following:
- Endocrine-Disrupting Chemicals: Endocrine-disrupting chemicals are substances present in plastics—such as bisphenol A or BPA, pesticides, and certain personal care products—that can interfere with hormone signaling by imitating or blocking estrogen and other reproductive hormones. Long-term exposure may impair ovarian function, speed up follicle depletion, and potentially cause earlier onset of menopause.
- Nutritional Deficiencies: Inadequate intake of key nutrients, such as vitamin D, B, zinc, and omega-3 fatty acids, can impair hormone production and ovarian health. Malnutrition or restrictive diets can contribute to irregular cycles and earlier menopause.
- Stress: Chronic stress triggers the hypothalamic-pituitary-adrenal or HPA axis, leading to elevated cortisol levels. Excess cortisol can inhibit gonadotropin-releasing hormone, thereby lowering LH and FSH activity and impairing ovarian function.
- Ovarian Reserve Depletion: The number of remaining eggs (ovarian reserve) naturally declines with age. Accelerated depletion—due to genetics, autoimmune issues, chemotherapy, or severe environmental or nutritional factors—can reduce estrogen production and lead to earlier menopause.
- Uterus Removal: Removing the uterus alone stops periods, but it does not immediately cause menopause, as the ovaries continue producing hormones. However, natural menopause may arrive earlier than expected.
- Certain Medical Conditions: Autoimmune diseases, such as thyroid disorders and rheumatoid arthritis, may cause the immune system to mistakenly attack the ovaries, reducing hormone production. Women with HIV may experience earlier menopause and more severe hot flashes. Chromosomal abnormalities, such as Turner syndrome, can lead to underdeveloped ovaries and early menopause. Additionally, women with myalgic encephalomyelitis or chronic fatigue syndrome may also have a higher risk of early or premature menopause.
- Medications: Certain medications can suppress menstruation and mask the natural timing of menopause, including hormonal contraceptives—such as combined hormonal contraceptives, progestin-only contraceptives, and long-acting reversible contraceptives—as well as gonadotropin-releasing hormone agonists and testosterone.
- Certain Cancer Treatments: Several cancer treatments may cause temporary or permanent menopause, including the following:
- Ovary Removal Surgery: Removing both ovaries (bilateral oophorectomy) causes immediate menopause, with a rapid drop in hormone levels and often more intense symptoms.
- Chemotherapy, Pelvic Radiation, and Hormone Therapy: These treatments can damage the ovaries and lead to temporary or permanent loss of menstrual periods and fertility. Younger women are less likely to experience permanent menopause.
- Smoking: Women who smoke often reach menopause up to two years earlier than nonsmokers and may have more severe symptoms.
- Family History: Women with a family history of early or premature menopause are more likely to experience it themselves.
Conversely, having multiple pregnancies may delay the onset of menopause.
For most women, menopause results from natural aging. In some cases, medical conditions or treatments may trigger it earlier or more abruptly.
[shortcut_anchor id=”anchor_1780096827407″ label=”Diagnosis”]How Is Menopause Diagnosed?[/shortcut_anchor]
For most women, menopause is recognized through changes in their menstrual cycle and symptoms alone, without formal testing. However, a clinical diagnosis may be needed for women with unclear menstrual patterns—such as those under 45, those who have had a hysterectomy (surgical removal of the uterus), those using hormonal treatments, or those with unusual symptoms—to confirm menopause and rule out other conditions.
Diagnosis is made retrospectively, when a woman has experienced 12 consecutive months without menstruation with no other explanation.
Additional tests or exams may be used in certain cases, including the following:
- Hormone Testing: Hormones such as FSH, estradiol, and LH may be tested in women under 45 with unexplained absence of periods.
- Pelvic Exam: Doctors may perform a pelvic exam to look for vaginal changes that support a menopause diagnosis or to evaluate symptoms such as dryness.
- Bone Density Test: Doctors may order this test to assess for osteoporosis. It is recommended for all women at age 65 if not done earlier.
During and after menopause, women should have regular physical, pelvic, breast, colorectal, and skin exams to monitor overall health.
[shortcut_anchor id=”anchor_1780096836224″ label=”Treatments”]What Are the Treatments for Menopause?[/shortcut_anchor]
Many women with mild symptoms choose not to seek medical treatment. All treatments carry potential side effects, and the right approach depends on symptom severity, medical history, and personal preference.
1. Hormone Therapy
Hormone therapy, also called hormone replacement therapy or HRT, is considered the most effective treatment for vasomotor symptoms. It replenishes estrogen and, for women with a uterus, progesterone helps protect against uterine cancer. It comes in different forms, including the following:
- Systemic Hormone Therapy: Pills, patches, or vaginal rings that relieve symptoms throughout the body. Patches may be preferred for women with a moderate risk of heart disease, while nonhormonal options may be recommended for those at higher risk of heart disease or breast cancer.
- Low-Dose Vaginal Products: Creams, tablets, capsules, or rings used locally to treat vaginal dryness, with fewer systemic effects. Side effects are uncommon but may include vaginal irritation or bleeding.
Several hormone therapies and products are currently available, including:
- Low-Dose Birth Control Pills: Provide contraception while also helping relieve menopausal symptoms and regulate irregular bleeding during the transition to menopause.
- Bioidentical Hormones: Lab-made hormones that are chemically identical to those produced by the body, and often called “natural” because they originate from plant sources. They are available in two forms:
- Pharmaceutical Bioidentical Hormone Products: These FDA-approved medications are used in standard menopausal hormone therapy and are regulated for quality and safety.
- Custom-Made Bioidentical Hormones: Mixed by pharmacies based on a doctor’s prescription to allow individualized dosing, tailored hormone combinations, and flexible delivery methods. However, although their individual ingredients are FDA-approved, with the exception of estriol, the compounded products are not FDA-regulated, may vary in quality and dosage, and may not be covered by insurance. Many women find bioidentical hormone therapies effective for relieving menopausal symptoms, and some believe they are safer than conventional hormone treatments. Patients should ensure that they use accredited pharmacies that provide verified lab testing.
Hormone therapy is generally appropriate for healthy women under 60, or within 10 years of menopause onset. It is not suitable for women who are pregnant or who have unexplained vaginal bleeding, certain cancers, a history of stroke or heart attack, blood clots, or liver disease.
For more than two decades, hormone therapy was framed as a simple yes-or-no decision—safe or dangerous. This oversimplification left many women without relief and others exposed to therapy without individualized guidance. In November 2025, the FDA removed the black-box warning from low-dose vaginal estrogen and softened the language for systemic therapy, signaling a shift toward personalized care.
Personalized hormone therapy emphasizes careful evaluation and ongoing adjustment. Clinicians are advised to run hormone metabolism tests, start with the lowest effective dose, choose the safest formulations, address underlying health factors, and reassess every six months.
2. Hormonal Supplement
Dehydroepiandrosterone or DHEA is an over-the-counter adrenal steroid hormone that is converted by the body into estrogen and androgens (hormones that drive male traits and reproductive development). When used as a vaginal suppository, it can help relieve vaginal dryness, atrophy, and pain during sexual intercourse.
3. Nonhormonal Prescription Medications
These medications are a suitable alternative for women who cannot use hormone therapy. Options include the following:
- Gabapentin: An antiseizure medication that can reduce hot flashes, particularly night sweats, and improve sleep when taken at bedtime.
- Selective Estrogen Receptor Modulators: Medications that mimic estrogen in specific tissues. Some reduce the risk of breast cancer and osteoporosis but don’t relieve hot flashes and may increase uterine cancer risk; others relieve vaginal dryness and painful intercourse; some combine with estrogen to relieve multiple menopausal symptoms and support bone health but may increase blood clot risk.
- Selective Serotonin Reuptake Inhibitors: Medications that may help manage mood swings, hot flashes, and sleep disturbances, with some evidence of greater effectiveness when combined with estrogen.
- Serotonin-Norepinephrine Reuptake Inhibitors: Medications that reduce the frequency and intensity of hot flashes and night sweats during menopause. They are particularly recommended for women who cannot use estrogen, such as those with a history of breast cancer.
4. Other Nonhormonal Treatments
Several conventional nonhormonal treatments can also effectively ease menopause-related symptoms.
Vaginal lubricants can reduce dryness and are generally available as short-acting or long-acting formulations. They can be water-, silicone-, or oil-based.
5. Clinical Hypnosis
A 2025 study of 250 postmenopausal women found that self-administered hypnotherapy significantly reduced hot flash frequency and severity by more than 50 percent, decreased daily disruption from menopausal symptoms, and was reported as highly beneficial.
6. Stellate Ganglion Blockade
This nonhormonal procedure involves injecting a local anesthetic near the stellate ganglion, a cluster of nerves in the neck that is part of the sympathetic nervous system. It has been studied as a treatment for severe hot flashes, especially in women who cannot use estrogen. A 2023 study of 35 perimenopausal women found significant reductions in hot flashes and improved sleep, although further research is needed to confirm its long-term benefits.
7. Herbal Medicines
Before trying any of the herbs listed below, you should consult your doctor or a qualified herbalist to check for potential interactions with your current medications or supplements.
- Ashwagandha: Ashwagandha contains compounds such as withanolides and alkaloids. Research published in January suggests it may improve mood, physical symptoms, and urogenital health, while reducing hot flashes and stress. Another 2021 study showed similar results, along with a significant decrease in FSH and LH hormones.
- Ayurvedic Shatavari Formulation: Shatavari has long been used in Ayurveda (traditional Indian medicine) as a medicinal plant to support women’s health. A 2025 study found that daily supplementation with shatavari or ashwagandha, alone or combined, helped reduce menopausal symptoms. Another 2024 study found that shatavari significantly reduced hot flashes, night sweats, insomnia, anxiety, vaginal dryness, and low libido.
- Black Cohosh: Traditionally used by Native Americans to help regulate menstrual cycles. Research suggests it mainly works through the brain to influence hormone levels and may support libido and bone health, although more research is needed.
- St. John’s Wort: Research suggests it may reduce the frequency, duration, and severity of hot flashes and improve mood and physical symptoms.
- Ginseng: A 2022 systematic review found that ginseng can help significantly reduce hot flashes, ease menopausal symptoms, and improve quality of life.
8. Acupuncture
A 2015 meta-analysis of 12 studies confirmed that acupuncture reduced the frequency and severity of hot flashes and improved other symptoms. Additional studies found improvements in vasomotor symptoms and quality of life, with benefits lasting at least six months after treatment ended, and another reported reductions in hot flash and night sweat frequency of up to 36 percent.
9. Biofeedback
Biofeedback uses electronic devices to provide real-time information about bodily processes, helping women learn to control pelvic muscle function. This approach may improve bladder control and reduce urinary symptoms.
[shortcut_anchor id=”anchor_1780096851274″ label=”Lifestyle Approaches”]What Are the Natural and Lifestyle Approaches to Menopause?[/shortcut_anchor]
There is an ongoing debate about the overmedicalization of menopause. Critics argue that framing it as a primarily medical problem—and emphasizing medications, supplements, and commercially marketed products—can overshadow education, lifestyle approaches, and individualized care. This may leave some women seeking unnecessary treatments or feeling anxious about a normal biological transition rather than feeling informed and empowered to manage symptoms based on their personal needs and preferences.
1. Diet
A nutrient-dense diet rich in protein, healthy fats, fruits, and vegetables supports overall health during menopause. Key foods include the following:
- Phytoestrogen-Rich Foods: Phytoestrogens are plant compounds that mimic estrogen, which may be helpful when hormone levels decline. The main types are isoflavones, found in soybeans, and lignans, found in flaxseed, whole grains, legumes, fruits, and vegetables.
- Calcium-Rich Foods: Adequate calcium, along with sufficient vitamin D, can help prevent bone loss and reduce the risk of fractures. Calcium-rich foods include dairy products, leafy greens such as bok choy and kale, almonds, broccoli, and canned fish with bones.
- Protein- and Collagen-Rich Foods: Protein supports muscles and bone strength. Good sources include eggs, chicken, and tofu. Foods that support collagen intake—such as bone broth, fish with skin, egg whites, organ meats, and seaweed—can also help support bones, muscles, and skin health.
2. Dietary Supplements
Several dietary supplements have been studied for their potential to support menopausal health and relieve symptoms without hormone therapy.
- Evening Primrose Oil: In a 2021 study involving 100 menopausal women, those who took evening primrose oil —two 1-gram capsules daily—experienced a significant improvement in menopausal psychological symptoms such as mood changes after two and four weeks, compared with a placebo group. Another 2021 study involving 170 participants found that evening primrose oil was effective in reducing the severity and frequency of night sweats.
- Berberine: This natural compound is found in plants such as Phellodendron, European barberry, and goldenseal. Research suggests that berberine may help reduce some of the negative effects caused by low estrogen levels, without the risks and side effects associated with hormone therapy.
- Maca Root: A processed form called pregelatinized maca has been linked to lower body weight and blood pressure, higher high-density lipoprotein (HDL) cholesterol and iron levels, and better hormone balance. Women taking maca have reported fewer hot flashes, less night sweating, better sleep, and improvements in mood and heart palpitations.
3. Exercises and Relaxation Techniques
Many women become less active during menopause due to fatigue and physical limitations, making regular movement especially important. Benefits include a healthy weight, better mood and sleep, stronger bones, lower risk of osteoporosis and heart disease, and improved cognitive function.
A balanced exercise routine should include aerobic activities for heart health, strength training for bone and muscle health, and flexibility exercises such as yoga or stretching for balance and mobility. Different types of exercise may work better for different women. Even 30 minutes of walking a day can help stabilize blood sugar, manage weight, and reduce hot flashes and sleep problems. Women with bladder control issues may also benefit from Kegel exercises, which involve tightening the pelvic muscles as if trying to stop the flow of urine.
Relaxation techniques—including meditation, deep breathing, muscle relaxation exercises, and paced breathing (slow abdominal breathing for about 15 minutes, twice a day)—may help manage anxiety and reduce the stress of hot flashes.
4. Other Lifestyle Modifications
Although lifestyle and behavioral changes may not eliminate symptoms, they can help reduce their effect.
- Avoid Triggers: Common triggers for hot flashes and night sweats include spicy foods, smoking, and alcohol.
- Use Cooling Strategies: Fans, air conditioning, breathable clothing, and cooling pillows or bedding can ease discomfort.
- Quit Smoking: Stopping smoking can help reduce hot flashes, as smoking worsens the symptom by increasing its severity and frequency.
- Maintain a Healthy Weight: Excess weight can worsen hot flashes.
- Stay Hydrated: Drinking enough water can help reduce hot flashes and keep your energy up, as it helps with body temperature regulation.
[shortcut_anchor id=”anchor_1780096862040″ label=”Mindset”]How Does Mindset Affect Menopause?[/shortcut_anchor]
Mindset does not change the underlying hormonal shifts of menopause, but it can influence how women experience and cope with symptoms. Psychological factors such as stress, anxiety, and beliefs about menopause can shape how symptoms such as hot flashes are perceived and how disruptive they feel. Research suggests that women who expect menopause to be very negative or stressful may report more severe or bothersome symptoms during the transition.
Interventions that address mindset, such as cognitive behavioral therapy and mindfulness, can also reduce the distress associated with menopausal symptoms and improve quality of life. These approaches help women develop coping strategies, manage stress, and change how they respond to symptoms, which can lessen their overall effect. However, while mindset can influence symptom perception and well-being, it does not replace medical treatments when they are needed.
[shortcut_anchor id=”anchor_1780096876339″ label=”Prevention”]How Can I Prevent Menopause?[/shortcut_anchor]
Menopause is a natural stage of life and cannot be prevented. However, women can lower their risk of long-term health conditions such as osteoporosis and heart disease by managing blood pressure and cholesterol, avoiding smoking, exercising regularly (especially strength training), and discussing bone health with their doctor as needed to determine whether calcium or vitamin D supplements may be beneficial.
Menopausal and postmenopausal women are also advised to have annual health checkups, including dental and eye exams, to help identify potential issues early, regardless of how healthy they feel. Regular mammograms are important because breast cancer risk rises with age. Most organizations recommend that women ages 45 to 54 undergo mammography every one to two years, with some guidelines suggesting annual screening and others allowing biennial screening.
[shortcut_anchor id=”anchor_1780096886566″ label=”Complications”]What Are the Possible Complications of Menopause?[/shortcut_anchor]
Menopause is a natural biological process rather than a disease, so its effects are typically described as health risks or consequences rather than complications. Many of these changes are linked to several long-term health effects, mainly due to a decline in ovarian hormone production, particularly estradiol.
- Metabolic Syndrome: Menopause is associated with a higher risk of metabolic syndrome, including increased abdominal fat, high blood pressure, and insulin resistance. This elevated risk often persists over time.
- Cardiovascular Disease: Menopause can accelerate changes in cardiovascular risk factors. During the transition, low-density lipoprotein cholesterol tends to rise, lipid profiles become less favorable, and changes in blood vessel function and elasticity may occur.
- Bone Health: Declining estrogen levels lead to reduced bone mineral density. Bone loss often begins during perimenopause and accelerates during late perimenopause and the first one to two years after the final menstrual period, with the greatest loss occurring within the first 10 years after menopause.
- Cognitive Changes: Some women may experience temporary changes in cognitive function during the menopausal transition. Cognitive function usually stabilizes or improves after menopause before gradually declining with age. Long-term cognitive decline is more closely linked to aging than to menopause itself.